
Bipolar disorder is one of the most complex psychiatric illnesses because it affects far more than mood alone. It is characterized by recurrent episodes of depression, mania, hypomania, or mixed states that alter emotional regulation, cognition, behavior, sleep, energy, motivation, and perception. Rather than representing simple fluctuations between happiness and sadness, bipolar disorder reflects a disruption in the brain’s ability to maintain emotional stability. Modern psychiatry recognizes it as a chronic neuropsychiatric condition involving genetic vulnerability, altered neural connectivity, circadian rhythm disturbances, and dysregulation of multiple neurotransmitter systems. Historically, bipolar disorder was known as manic-depressive illness. Although the terminology has changed, the central concept remains the same. The disorder involves pathological shifts between different mood states. However, these shifts are not always dramatic or predictable. Some individuals experience prolonged depressive episodes with only occasional hypomania. Others develop severe mania requiring hospitalization. Still others experience mixed episodes in which symptoms of depression and mania occur simultaneously. This variability contributes to the diagnostic complexity of the disorder. Depressive episodes often resemble major depressive disorder. Individuals experience persistent sadness, loss of interest, reduced energy, impaired concentration, hopelessness, guilt, changes in appetite, sleep disturbance, and, in severe cases, suicidal ideation. Because depression is frequently the first manifestation of bipolar disorder, many patients are initially diagnosed with unipolar depression. The underlying bipolar illness may remain undetected for years until a manic or hypomanic episode emerges. Mania represents the defining feature of bipolar disorder. It involves an abnormally elevated, expansive, or irritable mood accompanied by increased energy and goal-directed activity. Sleep requirements decrease dramatically. Some individuals function on only two or three hours of sleep while reporting no fatigue. Speech becomes rapid and difficult to interrupt. Thoughts accelerate. Attention shifts quickly from one idea to another. Confidence may increase to unrealistic levels, sometimes progressing into grandiose delusions. Risk-taking behaviors become common. Impulsive spending, reckless driving, substance misuse, and inappropriate sexual behavior may occur despite serious consequences. Not every manic episode appears euphoric. Many patients become predominantly irritable. Minor frustrations provoke disproportionate anger. Arguments become frequent. Impulsivity increases. Family relationships often deteriorate because the individual no longer recognizes the impact of their behavior on others. Hypomania resembles mania but occurs with lower intensity. Psychotic symptoms are absent. Daily functioning remains relatively preserved. Some individuals even describe hypomania as a period of exceptional productivity, creativity, or confidence. Because hypomania may feel pleasant rather than distressing, many patients fail to report it during psychiatric evaluation. This contributes significantly to delayed diagnosis. Mixed episodes illustrate the complexity of mood regulation. Patients may simultaneously experience hopelessness, guilt, suicidal thoughts, racing thoughts, agitation, insomnia, and increased energy. This combination represents one of the highest-risk clinical presentations because individuals possess both the despair associated with depression and the energy characteristic of mania. The biological basis of bipolar disorder extends beyond individual neurotransmitters. Earlier theories focused primarily on serotonin or dopamine deficiencies. Current neuroscience emphasizes abnormalities within large-scale neural networks regulating emotional processing, executive function, reward sensitivity, and circadian timing. Functional neuroimaging consistently demonstrates altered communication among the prefrontal cortex, amygdala, anterior cingulate cortex, hippocampus, and other limbic structures. These regions collectively regulate emotional stability. Disruption within these networks contributes to mood instability. Circadian rhythms play an especially important role. The brain relies upon internal biological clocks to regulate sleep, hormone secretion, body temperature, metabolism, and emotional function. Many individuals with bipolar disorder exhibit abnormalities in these rhythms. Sleep disruption often precedes manic episodes by several days. Reduced need for sleep is therefore not merely a symptom. It may actively contribute to mood destabilization. Maintaining regular sleep schedules has become an important component of long-term management. Genetics strongly influence bipolar disorder. Family and twin studies consistently demonstrate substantial heritability. However, inheritance is polygenic rather than deterministic. Multiple genes interact with developmental experiences, environmental stress, sleep patterns, substance use, and other biological factors. Possessing genetic vulnerability increases risk but does not guarantee illness. Environmental stressors frequently influence episode onset. Major life changes, interpersonal conflict, bereavement, occupational stress, sleep deprivation, childbirth, and psychoactive substances may trigger episodes in susceptible individuals. These events do not cause bipolar disorder independently. Instead, they interact with existing biological vulnerability. Cognition changes significantly across mood episodes. During depression, thinking becomes slow and pessimistic. Memory and concentration deteriorate. Decision-making becomes difficult. During mania, thinking accelerates but often loses organization. Ideas emerge rapidly, yet critical evaluation declines. Attention becomes easily distracted. Judgment weakens despite increased confidence. Even during periods of mood stability, some patients experience subtle impairments in executive functioning, verbal memory, or cognitive flexibility. Psychotic symptoms may occur during severe episodes. In mania, delusions commonly involve grandiosity, exceptional abilities, wealth, fame, or special missions. During depressive episodes, psychotic beliefs often revolve around guilt, worthlessness, punishment, or catastrophic illness. Hallucinations may also occur, although they are less common than mood-congruent delusions. Differential diagnosis remains challenging. Bipolar disorder shares symptoms with major depressive disorder, attention-deficit/hyperactivity disorder, borderline personality disorder, schizoaffective disorder, substance-induced mood disorders, and certain neurological conditions. Accurate diagnosis therefore requires careful longitudinal assessment rather than reliance upon a single clinical interview. Treatment aims not only to control acute episodes but also to prevent recurrence. Mood stabilizers remain the cornerstone of pharmacological management. Certain atypical antipsychotic medications also demonstrate effectiveness during acute mania and bipolar depression. Antidepressants require particular caution because, in some individuals, they may precipitate mania or accelerate mood cycling if prescribed without adequate mood stabilization. Psychotherapy complements pharmacological treatment. Psychoeducation helps patients recognize early warning signs of relapse. Cognitive-behavioral interventions improve coping strategies. Interpersonal and social rhythm therapy emphasizes stable daily routines, especially consistent sleep and activity patterns. Family-focused therapy improves communication and reduces interpersonal stress that may contribute to relapse. Recovery should not be understood as the permanent disappearance of symptoms. Instead, modern psychiatry views bipolar disorder as a lifelong condition requiring ongoing management. Many individuals achieve excellent occupational, academic, and interpersonal functioning when episodes are recognized early and treatment remains consistent. Adherence to medication, regular psychiatric follow-up, healthy sleep habits, avoidance of recreational drugs, and strong social
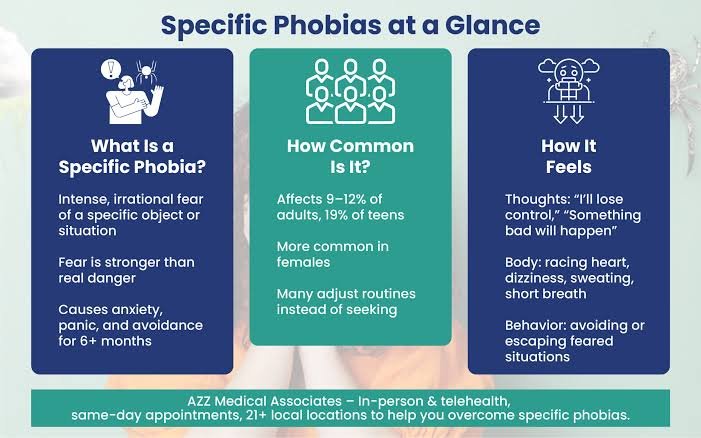
Why Do Phobias Feel So Real?
A phobia is far more than an ordinary fear. Nearly everyone experiences fear when confronted with genuine danger, but individuals with phobias develop intense anxiety in response to situations or objects that pose little or no objective threat. A harmless spider, a crowded elevator, an airplane, a needle, or even an open public space may provoke overwhelming panic. Despite recognizing that their fear is excessive, many individuals remain unable to control it. This apparent contradiction has made phobias one of the most fascinating subjects in psychiatry and neuroscience: why does the brain continue producing powerful fear even when logic clearly indicates safety? For many years, phobias were viewed primarily as learned emotional reactions. Although learning remains important, modern neuroscience demonstrates that phobias emerge through complex interactions among genetics, brain development, emotional regulation, memory, attention, and evolutionary survival mechanisms. Fear itself is not pathological. It is an adaptive biological response that has protected humans throughout evolution. Without fear, survival would have been impossible. The challenge arises when this protective system begins responding to harmless situations as though they represent life-threatening danger. The amygdala plays a central role in this process. Rather than functioning simply as a “fear center,” the amygdala continuously evaluates the emotional significance of incoming information. Its primary task is rapid threat detection. Importantly, the amygdala responds before conscious reasoning has fully evaluated the situation. This explains why individuals often experience fear before they have time to think logically. The emotional reaction precedes conscious interpretation. Evolution favored this arrangement because reacting too quickly occasionally was safer than reacting too slowly during genuine danger. Ordinarily, higher cortical regions gradually evaluate the situation. The prefrontal cortex compares current circumstances with previous experience, contextual information, and objective evidence. If no genuine danger exists, inhibitory signals reduce physiological arousal. In phobias, this regulatory process becomes less effective. The alarm system activates with extraordinary intensity, while corrective cognitive mechanisms struggle to reduce the response. As a result, the body behaves as though survival is immediately threatened. Heart rate accelerates. Breathing becomes rapid. Muscles tense. Sweating increases. Attention narrows. These physiological reactions are entirely real. Only the source of perceived danger differs from objective reality. Classical conditioning provides one explanation for phobia development. A frightening experience occurring in the presence of a neutral object may permanently associate that object with danger. A child bitten by a dog may later fear all dogs. A frightening experience during turbulence may contribute to fear of flying. However, many individuals develop phobias without remembering any traumatic event. This observation demonstrates that conditioning alone cannot explain every case. Observational learning also contributes. Children frequently acquire fears by watching caregivers. Repeated exposure to anxious parental reactions may teach the developing brain that certain situations deserve fear despite the absence of direct personal danger. Language further amplifies learning. Stories, media reports, warnings, and cultural beliefs all influence threat perception. The brain learns not only through personal experience but also through observation and communication. Evolutionary psychology offers another intriguing perspective. Some phobias develop far more easily than others. Fear of snakes, spiders, heights, darkness, or confined spaces occurs across many cultures. In contrast, people rarely develop equally intense phobias of electrical outlets, automobiles, or household appliances despite their greater objective danger. Researchers propose that the human brain evolved biological preparedness for threats commonly encountered throughout evolutionary history. Ancient dangers continue receiving preferential attention despite dramatic environmental change. Memory strongly influences phobic reactions. Emotional memories associated with fear become consolidated efficiently. Once established, these memories reactivate rapidly whenever similar situations arise. Importantly, each avoidance behavior prevents the brain from learning that the feared object is actually safe. Avoidance therefore maintains the disorder. The individual experiences temporary relief after escaping the feared situation. This relief reinforces future avoidance. Over time, fear gradually expands. A person avoiding one elevator may eventually avoid all elevators. One uncomfortable experience becomes generalized across increasingly broad situations. Attention becomes progressively biased toward detecting possible danger. Individuals with phobias continuously monitor the environment for feared stimuli. This hypervigilance increases the probability of noticing relevant cues while simultaneously reducing awareness of safety. The brain therefore receives disproportionate evidence supporting fear. Neutral experiences receive less attention. Threat-related information dominates conscious awareness. Predictive processing models have significantly advanced understanding of phobias. The brain continuously predicts future events before sensory information arrives. These predictions influence perception itself. Individuals with phobias begin anticipating danger long before encountering the feared object. The body prepares defensively in advance. Consequently, physiological symptoms often begin before objective exposure occurs. The individual interprets increased heart rate, dizziness, or muscular tension as evidence confirming danger. In reality, these bodily sensations result from anticipatory prediction rather than external threat. Interoception contributes another important mechanism. The brain constantly interprets signals originating within the body. Small physiological changes become amplified during anxiety. Normal increases in heart rate may appear alarming. Minor dizziness becomes interpreted catastrophically. This process creates reciprocal interaction. Fear produces bodily sensations. Those sensations increase fear. Greater fear intensifies physiological activation. The cycle reinforces itself. Not all phobias involve the same psychological mechanisms. Specific phobias usually involve clearly identifiable objects or situations. Social anxiety disorder centers upon fear of negative evaluation by others. Agoraphobia involves fear of situations in which escape or assistance might be difficult during panic-like symptoms. Although these disorders share common neurobiological features, each possesses distinctive cognitive patterns requiring individualized clinical understanding. Genetic influences also contribute significantly. Family studies demonstrate increased vulnerability among biological relatives. However, inheritance does not determine specific phobia content. Genes influence general sensitivity to fear, anxiety regulation, emotional learning, and stress responsiveness. Environmental experience shapes how these biological predispositions become expressed. Neuroimaging studies reveal altered communication among the amygdala, hippocampus, insular cortex, anterior cingulate cortex, and prefrontal regions. Rather than isolated abnormalities, phobias appear to involve dysregulated emotional networks. The amygdala detects threat rapidly. The hippocampus contributes contextual memory. The insula monitors bodily sensations. Executive regions evaluate evidence and regulate emotional responses. Successful treatment often strengthens communication among these systems rather than eliminating fear entirely.
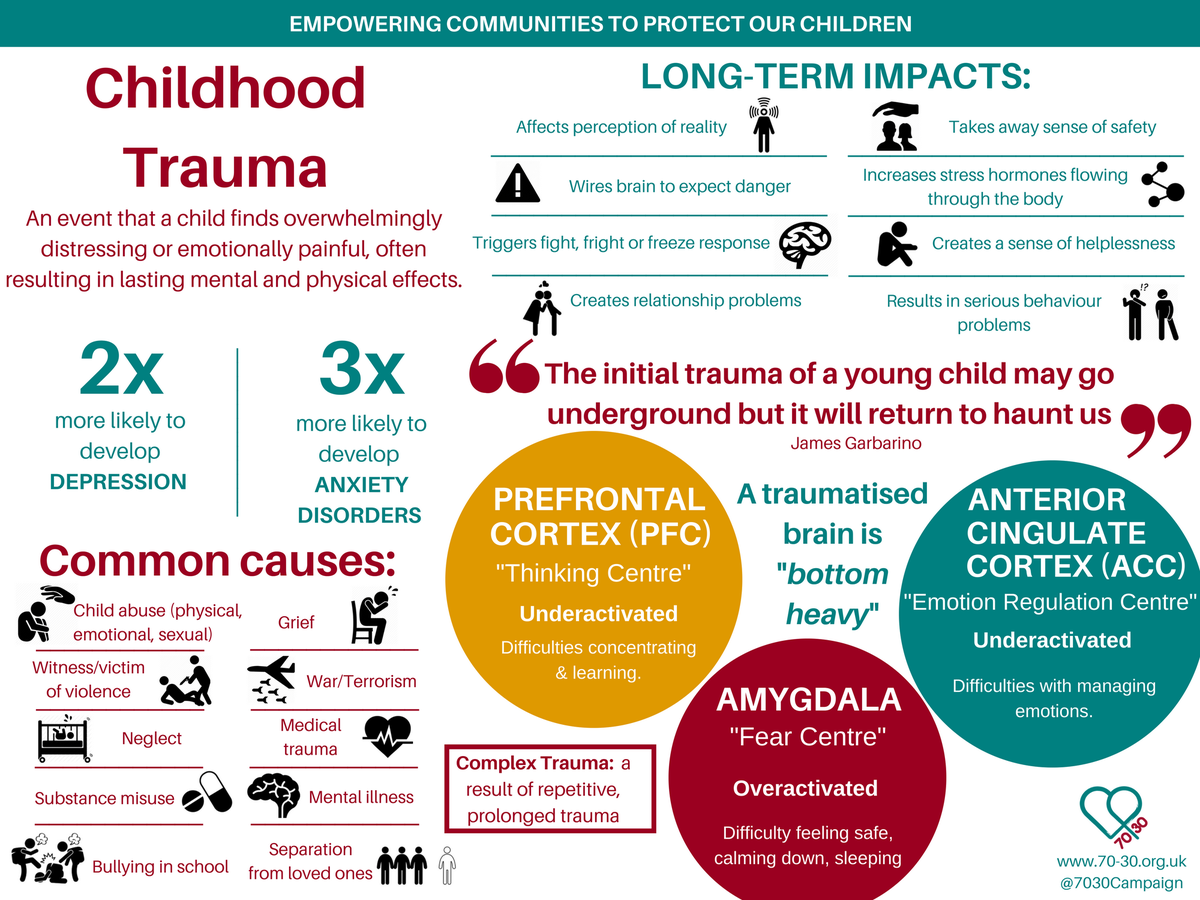
Why Do Childhood Traumas Last?
Childhood trauma is among the most extensively studied yet profoundly complex subjects in modern psychiatry. Unlike ordinary stressful experiences, psychological trauma occurring during childhood develops while the brain itself is still forming. During this period, neural circuits responsible for emotional regulation, memory, language, social cognition, stress adaptation, and self-identity remain highly plastic. Consequently, traumatic experiences do not simply become memories stored in the brain. They may actively influence the biological architecture through which future experiences are interpreted. This raises one of developmental psychopathology’s most important questions: why do childhood traumas continue affecting mental health decades after the original events have ended? For many years, trauma was understood primarily as an emotional wound. Contemporary neuroscience has expanded this perspective considerably. Childhood trauma represents not only a psychological experience but also a developmental event capable of influencing brain maturation, neuroendocrine regulation, immune function, cognitive development, and interpersonal attachment. The effects are therefore multidimensional. No single symptom defines childhood trauma. Instead, trauma may alter multiple psychological systems simultaneously. The developing brain differs fundamentally from the mature adult brain. During childhood, billions of neural connections are continuously strengthened, eliminated, and reorganized according to experience. This process allows extraordinary learning and adaptation. However, it also increases vulnerability. Repeated exposure to fear, unpredictability, neglect, abuse, or chronic emotional insecurity may influence which neural pathways become reinforced and which gradually weaken. The brain adapts to the environment in which it develops. When that environment is consistently threatening, survival becomes the primary developmental priority. From an evolutionary perspective, this adaptation is logical. A child growing up within dangerous circumstances benefits from heightened vigilance. Detecting subtle signs of anger, rejection, or violence may improve survival. The nervous system therefore becomes increasingly sensitive to potential threats. Attention shifts toward danger. Stress responses activate rapidly. Emotional regulation prioritizes protection over exploration. These adaptations may be highly effective during childhood. The difficulty emerges when the same biological strategies persist into adulthood after the environment has changed. The individual continues responding to ordinary situations as though danger remains imminent. One of the central biological systems involved is the hypothalamic-pituitary-adrenal axis. This neuroendocrine network regulates stress hormones throughout the body. Acute activation prepares the organism for immediate survival. Heart rate increases. Blood glucose rises. Attention narrows. Reaction time improves. Following resolution of danger, hormone levels ordinarily return to baseline. Chronic childhood trauma repeatedly activates this system. Over time, its regulation may become altered. Some individuals develop exaggerated stress responses. Others eventually demonstrate reduced physiological responsiveness following prolonged exposure. Both patterns reflect adaptation rather than simple dysfunction. Attachment theory provides another essential framework. Human infants depend upon caregivers not only for physical survival but also for emotional regulation. Before children can regulate their own emotions, caregivers perform this function externally. Consistent comfort teaches the developing nervous system that distress can be reduced safely. Unpredictable or frightening caregiving interferes with this learning. Instead of associating relationships with safety, children may associate intimacy with uncertainty, fear, or rejection. These early attachment patterns often influence interpersonal relationships throughout adult life. Importantly, attachment patterns are not permanent destinies. They represent developmental adaptations capable of changing through corrective relationships and therapeutic intervention. Memory develops differently under traumatic conditions. Ordinary autobiographical memories gradually become integrated into coherent life narratives. Traumatic experiences frequently resist this integration. Instead of being remembered as completed events located in the past, traumatic memories may remain fragmented into sensory impressions, bodily sensations, emotional reactions, or isolated images. Years later, seemingly harmless reminders may reactivate these fragments with remarkable intensity. The individual experiences emotions belonging to childhood while remaining physically present in adulthood. This phenomenon contributes significantly to post-traumatic symptoms. The amygdala plays an important role in threat detection throughout development. Repeated exposure to chronic stress may increase its sensitivity. Consequently, ambiguous situations become interpreted as potentially dangerous. Minor interpersonal conflict may evoke intense fear. Unexpected noises produce exaggerated startle responses. Neutral facial expressions appear threatening. These reactions often occur automatically before conscious reasoning has fully developed. Meanwhile, regions of the prefrontal cortex responsible for executive regulation continue maturing into early adulthood. Early adversity may influence communication between emotional and regulatory systems. The result is not simply stronger emotions but reduced capacity to modulate them effectively. This imbalance contributes to emotional dysregulation observed across numerous psychiatric disorders associated with childhood trauma. Identity formation also becomes profoundly affected. Children gradually develop beliefs regarding themselves through repeated interactions with caregivers and the surrounding environment. Consistent acceptance encourages secure self-concepts. Repeated criticism, neglect, humiliation, or abuse may gradually become incorporated into identity. Children rarely conclude that caregivers are fundamentally wrong. Instead, they often conclude that they themselves are fundamentally defective. These beliefs may persist for decades despite overwhelming contradictory evidence. Shame therefore becomes one of childhood trauma’s most enduring psychological consequences. Trauma influences cognition as well. Attention becomes biased toward detecting possible danger. Working memory may become overloaded by persistent vigilance. Decision-making increasingly prioritizes immediate safety rather than long-term goals. Learning becomes organized around avoiding harm. These cognitive adaptations often prove advantageous within threatening environments. Outside those environments, however, they may interfere with education, employment, relationships, and emotional well-being. Developmental psychopathology increasingly emphasizes cumulative rather than isolated adversity. Repeated emotional neglect, chronic criticism, domestic violence, bullying, parental mental illness, substance misuse within the family, or persistent insecurity may produce significant psychological effects even without catastrophic single events. Trauma therefore exists along a continuum. Severity depends not only upon the event itself but also upon developmental timing, duration, predictability, available support, genetic vulnerability, and opportunities for recovery. One particularly important concept is complex trauma. Unlike single-event trauma, complex trauma develops through prolonged interpersonal adversity during childhood. The resulting psychological profile often extends beyond fear alone. Individuals may experience chronic emotional dysregulation, unstable relationships, identity disturbance, persistent shame, dissociation, difficulties trusting others, and altered self-perception. Modern psychiatry increasingly recognizes complex trauma as distinct from traditional post-traumatic stress presentations. Epigenetic research has introduced another fascinating perspective. Traumatic experiences may influence patterns of gene expression without altering DNA sequences themselves. Environmental stress interacts continuously

Why Does Insight Disappear?
One of the most remarkable yet least understood phenomena in psychiatry is the loss of insight. Many psychiatric patients sincerely deny that anything is wrong despite displaying symptoms that are obvious to clinicians, family members, and even strangers. A person experiencing severe mania may insist they have never felt healthier while engaging in dangerous financial decisions, sleeping only two hours per night, and believing they possess extraordinary abilities. An individual with schizophrenia may firmly reject the suggestion that hallucinations are symptoms of illness, instead regarding them as undeniable reality. This raises a profound psychopathological question: why does the brain sometimes lose the ability to recognize its own dysfunction? At first glance, lack of insight appears to be simple denial. For decades, psychiatry often interpreted poor insight as a psychological defense against the emotional pain of accepting illness. Although psychological factors can influence self-awareness, modern neuroscience increasingly demonstrates that impaired insight is frequently a neurocognitive symptom rather than a voluntary refusal to acknowledge reality. The inability to recognize illness often reflects alterations within brain systems responsible for self-monitoring, error detection, and metacognition. Insight is considerably more complex than ordinary awareness. It requires several independent cognitive operations functioning simultaneously. The individual must notice unusual experiences. They must compare those experiences with previous functioning. They must recognize discrepancies. They must evaluate alternative explanations. Finally, they must conclude that the changes represent symptoms rather than ordinary reality. Failure at any stage may reduce insight. Consequently, insight should not be understood as a single ability. It is the product of multiple interacting cognitive systems. One of the central concepts in contemporary psychiatry is metacognition. Metacognition refers to the capacity to think about one’s own thinking. The brain continuously evaluates its own beliefs, memories, emotions, perceptions, and decisions. Healthy metacognition allows individuals to question conclusions, revise opinions, recognize mistakes, and acknowledge uncertainty. Without this capacity, beliefs become increasingly resistant to correction. In psychotic disorders, metacognitive processes often become significantly disrupted. The brain continues generating interpretations of experience. However, its ability to evaluate the accuracy of those interpretations becomes impaired. This distinction explains why delusions remain so convincing. Patients are not simply choosing incorrect beliefs. Their internal systems responsible for questioning those beliefs are functioning differently. Neuroimaging studies suggest that insight depends upon communication among distributed brain networks rather than isolated regions. The prefrontal cortex contributes executive monitoring and cognitive flexibility. The anterior cingulate cortex participates in detecting conflict between expectations and incoming information. The insular cortex integrates internal bodily awareness with emotional significance. Parietal regions contribute self-representation. Together these systems continuously update the individual’s understanding of themselves. Disruption within these networks may impair awareness of illness without affecting many other intellectual abilities. This explains why highly intelligent individuals may nevertheless lack insight into severe psychiatric symptoms. General intelligence and self-awareness rely upon overlapping but distinct neural mechanisms. One particularly important concept involves prediction error. The brain constantly predicts what should happen next. When reality differs from expectation, prediction errors signal that internal models require updating. Healthy cognition depends upon these signals. If prediction error processing becomes altered, incorrect beliefs may persist despite contradictory evidence. The individual no longer experiences sufficient internal pressure to revise existing explanations. Consequently, pathological beliefs become increasingly stable. This mechanism has received considerable attention in schizophrenia research. Patients often experience highly unusual perceptions or thoughts. Ordinarily, such experiences would trigger doubt. Instead, altered prediction systems may encourage certainty. The strange experience itself becomes accepted as genuine evidence. Alternative explanations receive progressively less consideration. Insight therefore deteriorates not because evidence disappears but because evidence is interpreted differently. Mood disorders provide another perspective. Insight varies considerably across different emotional states. During severe depression, many patients possess excessive rather than diminished insight. They evaluate themselves with extraordinary harshness. Failures appear permanent. Achievements seem insignificant. The future feels hopeless. Interestingly, these conclusions often feel objectively accurate despite being heavily influenced by depressive cognition. This phenomenon has led some researchers to distinguish factual awareness from emotional realism. Depression alters both. Mania presents the opposite pattern. Confidence increases dramatically. Self-criticism decreases. Limitations appear insignificant. Risk assessment becomes impaired. Because elevated mood itself influences judgment, patients frequently interpret pathological energy as exceptional health. Reduced need for sleep appears advantageous. Impulsive spending feels rational. Grandiose plans seem entirely achievable. From the patient’s perspective, concern expressed by others often appears unnecessary or obstructive. Anosognosia represents one of the most striking neurological examples of impaired insight. Following certain forms of brain injury, patients may completely deny obvious physical disabilities. Some insist they can move paralyzed limbs despite objective inability. Others reject clear evidence of blindness or weakness. Importantly, these individuals are not intentionally lying. Their brains genuinely fail to construct awareness of impairment. Psychiatry increasingly recognizes similarities between neurological anosognosia and impaired insight observed in severe mental illness. Both suggest that self-awareness depends upon specific neural mechanisms capable of dysfunction. Memory contributes significantly as well. Insight requires comparing present functioning with previous experience. If autobiographical memory becomes altered or selectively interpreted, recognizing change becomes increasingly difficult. Patients may reinterpret previous symptoms according to current beliefs. Psychotic episodes become viewed as spiritual experiences. Manic behaviors become remembered as periods of exceptional productivity. Depressive episodes become interpreted as evidence of personal weakness rather than illness. Memory reconstruction therefore influences self-awareness continuously. Social cognition also affects insight. Human beings ordinarily evaluate themselves partly through interaction with others. Family members, friends, and colleagues provide continuous external feedback. Psychiatric illness frequently disrupts these relationships. Social withdrawal reduces corrective feedback. Paranoia decreases trust. Grandiosity dismisses criticism. The individual gradually loses access to external perspectives capable of challenging internal interpretations. Consequently, self-awareness becomes increasingly dependent upon distorted internal models. The relationship between insight and treatment adherence is profound. Patients who do not recognize illness frequently question the necessity of medication or psychotherapy. This creates one of psychiatry’s greatest clinical challenges. Nonadherence often reflects impaired awareness rather than deliberate refusal. Recognizing this distinction changes the therapeutic approach. Confrontation rarely improves insight. Instead, collaborative communication, psychoeducation, therapeutic alliance, and gradual
Can the Brain Create False Memories?
Memory is often regarded as one of the most reliable functions of the human mind. People commonly assume that important experiences are stored within the brain much like files within a computer, waiting to be retrieved whenever needed. This belief feels intuitively correct because memories often possess remarkable vividness and emotional certainty. Yet one of the most important discoveries in modern cognitive neuroscience is that memory is not a recording system. It is a reconstructive process. Every act of remembering involves rebuilding the past rather than replaying it exactly as it occurred. This realization has transformed psychology, psychiatry, and neuroscience by raising a profound question: can the brain create memories of events that never actually happened? The answer, supported by decades of scientific research, is yes. False memories are genuine subjective experiences. Individuals who possess them are usually not lying, pretending, or intentionally distorting reality. Instead, the brain reconstructs past events in ways that may unintentionally incorporate inaccurate details, altered interpretations, or entirely imagined experiences. The resulting memory often feels just as convincing as an accurate one. Understanding this phenomenon requires abandoning the traditional view of memory as permanent storage. Whenever an experience occurs, the brain does not preserve every detail equally. Instead, it selectively encodes information according to attention, emotional significance, existing knowledge, expectations, and biological state. Only portions of the original experience become stabilized. Many details are never stored at all. When people later remember an event, the brain fills missing information using previous knowledge, contextual expectations, emotional associations, and logical inference. Most of the time this reconstruction produces memories that are sufficiently accurate for everyday life. Occasionally, however, reconstruction introduces substantial error. The hippocampus plays a central role in this process. Rather than functioning as a storage location, the hippocampus helps organize experiences into coherent episodic memories. It binds together sensory information, spatial context, emotional responses, temporal sequence, and personal significance. Later recollection depends upon reactivating these distributed neural representations. Importantly, each retrieval changes the memory itself. This process, known as reconsolidation, represents one of the most significant findings in modern memory research. Contrary to earlier assumptions, recalling a memory temporarily makes it biologically unstable. Before returning to long-term storage, it undergoes reconsolidation. During this period, new information may become incorporated. Interpretations may change. Emotional meaning may shift. Even subtle suggestions can influence future recollections. Consequently, remembering is simultaneously an act of preservation and modification. This explains why memories gradually evolve across years despite the individual’s confidence that they remain unchanged. Emotion profoundly influences these mechanisms. Highly emotional experiences are often remembered more vividly than ordinary events. However, vividness does not necessarily indicate accuracy. Stress hormones strengthen memory for central emotional themes while frequently reducing peripheral detail. During traumatic experiences, attention narrows toward immediate survival. Later recollection may therefore contain exceptionally vivid fragments alongside major gaps in contextual information. This pattern contributes to the fragmented nature of many traumatic memories. Contemporary psychiatry emphasizes that traumatic memory should not be understood simply as stronger memory. Rather, it often differs qualitatively from ordinary autobiographical recollection. False memories emerge through multiple pathways. One involves suggestion. Repeated exposure to misleading information gradually alters reconstruction. Another involves imagination. Repeatedly imagining an event increases familiarity. Over time, familiarity itself may become interpreted as evidence that the event actually occurred. The distinction between imagining and remembering becomes increasingly difficult to identify. This process occurs because both imagination and episodic memory activate overlapping neural networks. The brain does not maintain completely separate systems for reality and simulation. Instead, similar mechanisms contribute to both. Developmental psychology demonstrates that children are particularly susceptible to suggestion because memory systems remain immature. However, adults are by no means immune. Confidence should never be equated with accuracy. Individuals frequently express complete certainty regarding memories later demonstrated to be objectively incorrect. This discrepancy illustrates one of memory’s central paradoxes. Subjective certainty reflects current neural reconstruction rather than historical truth. Eyewitness testimony provides striking examples. Legal systems have traditionally regarded confident eyewitnesses as highly reliable. Psychological research has repeatedly challenged this assumption. Stress, expectation, attention, lighting, suggestion, social influence, and repeated questioning all influence recollection. Mistaken identification has contributed to numerous wrongful convictions subsequently overturned by DNA evidence. These findings have profoundly influenced forensic psychology. Memory contamination does not require malicious intent. Ordinary conversation may gradually reshape recollection. Family members discussing childhood experiences often influence one another’s memories without recognizing it. Details borrowed from photographs, stories, or other people’s accounts become incorporated into personal autobiographical narratives. Eventually, individuals experience these reconstructed memories as direct recollections. Psychiatric disorders illustrate additional complexity. Major depression biases autobiographical memory toward negative interpretation. Anxiety enhances memory for perceived threat. Post-traumatic stress disorder increases involuntary retrieval of emotionally significant fragments. Psychotic disorders may occasionally involve false autobiographical beliefs arising from broader disturbances in reality monitoring. Each condition influences reconstruction differently. Reality monitoring represents another crucial cognitive function. The brain continuously determines whether information originated from direct perception, imagination, dreams, conversations, or internal thought. Healthy cognition performs this distinction remarkably efficiently. Occasionally, however, source monitoring errors occur. An imagined conversation becomes remembered as real. A dream acquires qualities of autobiographical experience. A fictional story becomes confused with personal history. Most individuals experience minor source monitoring errors throughout life. In psychopathology, these mechanisms may become substantially more vulnerable. Neuroscientific investigations increasingly emphasize predictive processing. The brain reconstructs memory partly by predicting what most likely occurred. Predictions arise from previous experience, cultural knowledge, emotional expectations, and statistical regularities. Most predictions prove highly useful. However, they also introduce systematic biases. Events consistent with expectations become easier to remember. Unexpected details become vulnerable to omission or alteration. Memory therefore reflects interaction between historical events and predictive reconstruction. This principle explains why stereotypes may unconsciously influence recollection. Expected information receives stronger cognitive support than unexpected information. Sleep contributes significantly to memory accuracy. During sleep, recently acquired information undergoes consolidation. Neural representations become reorganized and integrated with existing knowledge. Insufficient sleep impairs these processes. Memory becomes less detailed, less stable, and increasingly susceptible to
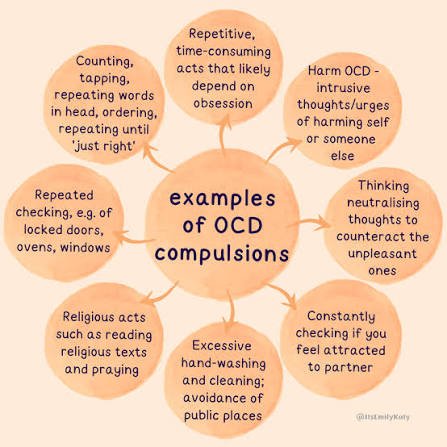
Why Do Thoughts Become Obsessions?
Among the most fascinating questions in modern psychiatry is why the human brain sometimes becomes unable to release a single thought. Every healthy mind produces countless unwanted ideas throughout the day. Violent images, inappropriate words, irrational fears, embarrassing memories, and bizarre possibilities briefly enter consciousness before disappearing almost immediately. Most people hardly notice them. Yet in obsessive-compulsive disorder (OCD), these same ordinary mental events become persistent, emotionally overwhelming, and nearly impossible to ignore. The central mystery is not why intrusive thoughts exist—they occur in nearly everyone—but why certain brains assign extraordinary importance to thoughts that would otherwise be dismissed. For decades, obsessive thoughts were misunderstood as evidence of unusual personality traits or hidden unconscious desires. Contemporary psychiatry has largely abandoned these explanations. Research increasingly demonstrates that obsessions arise from abnormalities in cognitive control, uncertainty processing, threat detection, emotional regulation, and neural circuits responsible for evaluating significance. The problem is not that individuals with OCD think differently from everyone else. The problem is that their brains respond differently to the same kinds of thoughts experienced by the general population. The first principle in understanding obsessions is recognizing that the brain continuously filters information. Every second, countless thoughts, sensations, memories, and perceptions compete for conscious attention. Most are automatically discarded. This filtering system allows attention to remain focused on information that is genuinely important. Without it, consciousness would become overwhelmed by irrelevant mental activity. In OCD, this filtering process appears to malfunction. Instead of allowing intrusive thoughts to pass naturally, the brain repeatedly identifies them as highly significant. A random thought such as “Did I lock the door?” no longer remains an ordinary question. It becomes an unresolved threat. The mind begins treating uncertainty itself as danger. Modern neuroscience suggests that this process involves abnormal activity within cortico-striato-thalamo-cortical circuits. These interconnected brain networks help regulate decision-making, error detection, habit formation, and behavioral inhibition. Rather than switching attention away from completed concerns, these circuits continue signaling that something remains unresolved. The result is a persistent internal message that the task is incomplete. Even when objective evidence clearly indicates safety, the brain continues generating doubt. This persistent doubt represents one of OCD’s defining characteristics. Patients rarely seek absolute certainty because they enjoy certainty. They seek it because their nervous system struggles to tolerate uncertainty itself. The emotional experience becomes so uncomfortable that repeated checking, washing, counting, or reassurance temporarily reduces distress. Unfortunately, this relief is short-lived. Each ritual teaches the brain that the obsession deserved attention. Consequently, future intrusive thoughts become even more convincing. A self-reinforcing cycle develops. Compulsions therefore do not merely accompany obsessions. They strengthen them. Another remarkable feature of OCD is thought-action fusion. Many patients gradually begin experiencing thoughts as morally or physically equivalent to actions. An intrusive image of harming someone may feel almost as disturbing as actually committing violence. The individual recognizes intellectually that no action has occurred. Emotionally, however, guilt and responsibility remain overwhelming. This explains why people with OCD are often among the least likely individuals to act upon their intrusive thoughts. The thoughts themselves are profoundly inconsistent with their values. Precisely because they care deeply about preventing harm, the brain becomes trapped monitoring every possible threat. Neuroimaging studies reveal that regions involved in error monitoring frequently show increased activity in OCD. The brain behaves as though mistakes are constantly about to occur. Even ordinary uncertainty activates systems normally reserved for genuine danger. This exaggerated error signal influences virtually every aspect of cognition. Simple decisions become exhausting. Completed tasks continue feeling unfinished. Reassurance loses effectiveness because the internal warning system remains active. The person is not searching for information. They are searching for a feeling of certainty that never fully arrives. Memory is also affected. Contrary to popular assumptions, many individuals with OCD possess intact or even excellent memory. The difficulty lies not in remembering but in trusting memory. Repeated checking gradually weakens confidence. After verifying a locked door multiple times, individual checking episodes become difficult to distinguish. Memory becomes less vivid precisely because the behavior has been repeated excessively. The resulting uncertainty encourages further checking. Again, the disorder maintains itself through recursive learning. One of the most important developments in contemporary psychiatry involves predictive processing models. The brain continuously predicts what should happen next and updates these predictions according to incoming evidence. In OCD, prediction systems appear unusually sensitive to low-probability negative outcomes. Tiny possibilities receive disproportionate attention. Although the individual recognizes that catastrophe is unlikely, the nervous system behaves as though unlikely events require immediate prevention. This explains why logical reassurance often provides limited benefit. The difficulty lies within predictive learning rather than factual knowledge. Emotion plays a central role throughout this process. Obsessions persist not because they contain important information but because they acquire intense emotional salience. Fear, guilt, disgust, responsibility, and uncertainty combine to create unusually powerful learning signals. The brain mistakenly concludes that emotionally intense thoughts must also be objectively important. In reality, emotional intensity and factual significance are not equivalent. Developmental experiences may influence vulnerability as well. Genetic factors contribute substantially to OCD risk, yet environmental learning shapes symptom content. Children raised in highly unpredictable or excessively responsibility-focused environments may become particularly sensitive to uncertainty. However, OCD cannot be explained solely through upbringing. Twin studies consistently demonstrate significant biological contributions involving multiple genes interacting with developmental experiences. One particularly fascinating observation is that obsessional themes vary across cultures while underlying mechanisms remain remarkably similar. Some individuals fear contamination. Others fear blasphemy. Others become preoccupied with symmetry, morality, illness, sexuality, relationships, or memory. Despite these differences, the underlying psychological architecture remains consistent. An intrusive thought becomes assigned excessive significance. Uncertainty becomes intolerable. Compulsive behavior temporarily reduces distress. Negative reinforcement strengthens the cycle. Modern treatment reflects this understanding. Exposure and response prevention therapy gradually teaches the brain that uncertainty can be tolerated without performing compulsions. Rather than proving feared outcomes impossible, therapy reduces the perceived necessity of achieving perfect certainty. Over time, neural learning begins changing. The internal alarm system gradually becomes
Why Does Reality Feel Unreal?
One of the most disturbing experiences described in psychopathology is the sudden feeling that the world has somehow become unreal. Individuals often report that familiar places appear artificial, loved ones seem emotionally distant, mirrors feel strangely unfamiliar, and ordinary life resembles a dream or a film. Despite recognizing intellectually that nothing has actually changed, they cannot escape the overwhelming sensation that reality itself has become fundamentally different. This phenomenon, known clinically as derealization and often accompanied by depersonalization, represents one of the most intriguing disorders of conscious experience. Unlike psychosis, derealization does not involve losing contact with reality. Most individuals understand that the external world remains objectively unchanged. The conflict exists between knowledge and experience. They know their surroundings are real, yet they no longer feel real. This distinction is central to modern psychiatry because it reveals that conscious reality consists of more than accurate perception alone. Reality also requires emotional familiarity, bodily integration, and the continuous sense of presence generated by the brain. For decades, psychiatrists struggled to explain why this phenomenon occurs. Earlier theories emphasized psychological defense mechanisms, suggesting that the mind temporarily distances itself from overwhelming emotional pain. Although trauma remains an important contributor, contemporary neuroscience demonstrates that derealization cannot be understood solely through psychological explanations. Functional brain imaging increasingly reveals alterations within networks responsible for emotional processing, attention, self-awareness, and sensory integration. The brain continuously constructs the feeling that the surrounding world is meaningful and emotionally significant. Visual information alone is insufficient to create reality. Every object people perceive simultaneously activates emotional associations, autobiographical memories, expectations, bodily responses, and predictions regarding future interaction. A familiar home does not appear meaningful merely because it is recognized visually. It feels familiar because multiple neural systems simultaneously assign emotional relevance to what is being perceived. Derealization appears to disrupt this integration. Visual perception often remains remarkably accurate. Memory remains largely intact. Reasoning frequently remains normal. What changes is emotional registration. The environment loses its ordinary sense of familiarity. People often describe the world as flat, distant, silent, colorless, or strangely artificial despite seeing exactly the same physical surroundings. Modern neuroscience suggests that emotional overregulation plays an important role. During overwhelming stress or trauma, defensive neural systems may reduce emotional intensity to protect the individual from unbearable psychological pain. This adaptation can be lifesaving during extreme situations. However, when the mechanism persists beyond immediate danger, emotional blunting begins affecting ordinary perception. Reality no longer feels emotionally connected because emotional processing itself has been reduced. The nervous system, in effect, protects the individual by decreasing emotional access to experience. Unfortunately, this protective strategy also diminishes the feeling of being fully alive. Many individuals first experience derealization during panic attacks. As physiological arousal rises rapidly, attention shifts inward toward bodily sensations. Heartbeat, breathing, dizziness, and muscular tension become the primary focus of awareness. External reality gradually receives less attentional processing. The surrounding environment may consequently begin feeling distant or dreamlike. Importantly, the derealization itself often intensifies panic. Individuals become frightened by the sensation that they are losing their minds. This fear increases physiological arousal. Greater arousal strengthens dissociative symptoms. A self-perpetuating cycle gradually develops. One of the most fascinating discoveries involves predictive processing. According to contemporary computational neuroscience, perception depends heavily upon predictions generated before sensory information arrives. The brain continuously anticipates what reality should feel like. These predictions include not only visual expectations but also emotional expectations. When emotional signals become weakened, prediction systems receive incomplete information. The resulting mismatch contributes to the strange feeling that something fundamental has changed. The world appears visually identical while simultaneously lacking its expected emotional quality. The brain detects inconsistency but struggles to explain it. This contributes to the unsettling conviction that reality itself has somehow shifted. Sleep deprivation offers another important clue. Many healthy individuals experience brief derealization after prolonged lack of sleep. Fatigue alters communication among attention networks, emotional systems, and executive regions responsible for maintaining coherent conscious experience. Similar alterations occur during severe stress, chronic anxiety, and certain neurological disorders. These observations suggest that derealization represents a disturbance in large-scale brain integration rather than damage to a single structure. The default mode network has attracted considerable attention in recent years. This network contributes to self-referential thinking, autobiographical reflection, and the continuous experience of personal identity. Abnormal communication between the default mode network and systems responsible for external attention may contribute to dissociative symptoms. When internal and external awareness become poorly synchronized, both the self and the surrounding world may begin feeling unfamiliar. This relationship explains why derealization frequently occurs alongside depersonalization. The individual simultaneously feels disconnected from the environment and from themselves. Memory also influences these experiences in subtle ways. Reality normally feels continuous because present perception automatically connects with autobiographical knowledge. Every familiar street, voice, or object activates countless previous experiences stored throughout life. During derealization, these emotional connections appear weakened. Recognition remains intact. Emotional familiarity decreases. The result resembles meeting someone whose face is instantly recognizable yet somehow emotionally unfamiliar. The experience is profoundly unsettling precisely because logical knowledge and emotional experience no longer agree. Developmental experiences may increase vulnerability. Individuals exposed to chronic childhood trauma often develop highly sensitive defensive systems. Dissociation becomes an adaptive strategy allowing continued psychological functioning despite overwhelming environments. Years later, the same defensive mechanisms may activate automatically during stress even when objective danger no longer exists. The adult nervous system continues using strategies originally developed for childhood survival. This perspective has significantly influenced trauma-informed psychiatry. Rather than viewing dissociation as evidence of weakness or irrationality, clinicians increasingly recognize it as an adaptive biological response that persists beyond its original context. Pharmacological research remains complex. No medication specifically eliminates derealization in every patient. Instead, treatment generally targets underlying conditions such as anxiety disorders, depression, post-traumatic stress disorder, or obsessive-compulsive disorder. Psychotherapy often focuses upon reducing chronic hyperarousal, improving emotional regulation, strengthening present-moment awareness, and gradually reducing fear associated with dissociative experiences. Perhaps the greatest challenge lies in the patient’s interpretation of symptoms. Many individuals become convinced they
How Does the Brain Shape Human Speech?
Speech is one of the most sophisticated functions of the human brain. Every spoken sentence requires the precise coordination of billions of neurons responsible for language, memory, attention, hearing, breathing, movement, emotion, and executive control. Although speaking feels effortless for most people, it is actually the result of one of the most complex neurological processes known to science. When even a small part of this system is disrupted, speech may become slow, unclear, fragmented, repetitive, or completely absent. For this reason, speech disorders are not simply problems of pronunciation or communication; they often reflect deeper alterations in brain function. For many years, researchers believed that language was controlled primarily by two isolated brain regions. Modern neuroscience has dramatically expanded this understanding. Speech is now viewed as the product of large-scale neural networks rather than a single language center. Multiple regions continuously exchange information within milliseconds, allowing thoughts to become words and words to become coordinated movements of the lips, tongue, jaw, vocal cords, and respiratory muscles. The process begins long before the first word is spoken. Every conversation starts with an intention. The brain must first determine what it wishes to communicate. Executive regions within the frontal cortex organize goals, select relevant information, inhibit unnecessary thoughts, and prepare a communicative plan. Only after this planning stage does language processing begin. One of the most important language regions is Broca’s area, located in the frontal lobe. Rather than storing words, this region helps organize the motor patterns necessary for producing speech. It coordinates grammar, sentence construction, and the sequencing of movements required for articulation. Damage to this area often produces slow, effortful speech in which individuals know exactly what they want to say but struggle to produce fluent language. This condition is known as expressive aphasia. Another critical region is Wernicke’s area within the temporal lobe. This area contributes primarily to language comprehension. Individuals with damage here may continue speaking fluently, yet their sentences become difficult or impossible to understand because word selection and meaning are profoundly disrupted. Remarkably, many patients remain unaware that their speech has become incomprehensible. This demonstrates that producing language and monitoring language depend upon partially separate neural systems. Communication between these regions is equally important. Nerve pathways connecting frontal and temporal language networks allow comprehension and speech production to function as an integrated system. Damage to these connecting fibers may result in conduction aphasia, a disorder in which individuals understand speech and speak relatively fluently but experience major difficulty repeating words or correcting verbal mistakes. Speech also depends heavily on the motor cortex. Every spoken sound requires highly coordinated activation of muscles controlling the tongue, lips, palate, vocal folds, and diaphragm. These movements occur within fractions of a second and must remain precisely synchronized. Even minor disruption of motor pathways can significantly affect articulation. The cerebellum, traditionally associated with balance and movement, plays a surprisingly important role in speech as well. It fine-tunes timing, coordination, rhythm, and precision. Damage to the cerebellum often produces scanning speech, in which words become slow, irregular, and poorly coordinated despite intact language knowledge. The basal ganglia contribute another essential component. These deep brain structures regulate the initiation and smooth execution of movement. Disorders affecting the basal ganglia, such as Parkinson’s disease, frequently produce reduced vocal volume, monotonous speech, slowed articulation, and difficulty initiating verbal communication. Although language itself remains largely intact, the motor execution of speech becomes impaired. Speech also depends upon intact auditory processing. People constantly monitor their own voices while speaking. The auditory cortex compares expected sounds with actual vocal output, allowing continuous correction of pronunciation, rhythm, and volume. Without this feedback system, speech gradually becomes less accurate. This explains why hearing loss can significantly influence speech production over time. Memory systems are equally involved. Semantic memory stores vocabulary and factual knowledge, while working memory temporarily holds words during conversation. Every sentence requires continuous interaction between long-term language knowledge and short-term information processing. Disorders affecting working memory often produce interrupted speech, frequent pauses, and difficulty completing complex sentences. Attention represents another fundamental component. Fluent conversation requires maintaining focus while simultaneously selecting appropriate words, suppressing irrelevant thoughts, monitoring listeners’ reactions, and preparing future responses. Conditions that impair attention, including attention-deficit disorders, traumatic brain injury, and certain psychiatric illnesses, may therefore produce noticeable communication difficulties even when language itself remains preserved. One of the most fascinating discoveries in modern neuroscience concerns predictive processing during speech. The brain does not simply react while speaking. Instead, it continuously predicts upcoming sounds before they are produced. These predictions allow extraordinarily rapid correction of minor errors without conscious awareness. Most people adjust pronunciation automatically because the brain constantly compares intended speech with actual output. Stuttering provides an important example of how these predictive systems may become disrupted. Although the precise neurological mechanisms remain under investigation, research suggests that altered timing within brain networks responsible for speech planning, motor coordination, and auditory feedback contributes to dysfluency. Stuttering is therefore not simply a habit or psychological problem. It reflects differences in how the brain coordinates the complex timing required for fluent speech. Emotional stress often worsens symptoms, but stress does not cause the underlying neurological vulnerability. Developmental speech disorders further illustrate the complexity of brain-language relationships. Children acquire speech through gradual maturation of neural networks interacting with environmental experience. Genetic factors, auditory input, motor development, and social communication all contribute. Delays in any of these processes may influence language acquisition, although many children eventually achieve normal communication through continued brain development and appropriate intervention. Traumatic brain injury represents another important cause of speech impairment. Depending on the location and severity of injury, individuals may experience aphasia, dysarthria, apraxia of speech, or broader cognitive-communication disorders. Dysarthria results from weakness or poor coordination of speech muscles, while apraxia of speech reflects difficulty planning voluntary speech movements despite normal muscle strength. These disorders demonstrate that successful communication depends upon multiple independent neurological systems functioning together. Stroke remains one of the most common neurological causes of acquired speech disorders.
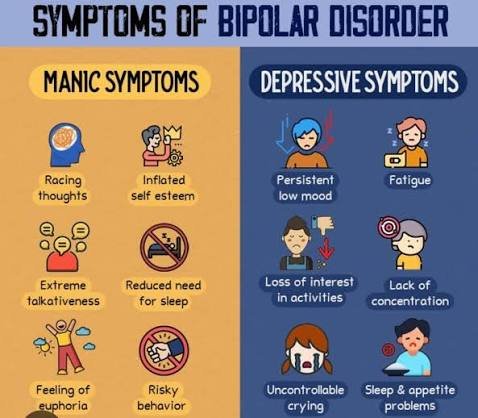
Can Mania Hide Behind Depression?
Among all psychiatric disorders, few are as misunderstood as bipolar disorder, historically referred to as manic-depressive illness. Many people assume that bipolar disorder simply involves alternating periods of happiness and sadness. Modern psychiatry demonstrates that this description is profoundly inaccurate. Mania is not merely an elevated mood, and depression is not simply intense sadness. Both represent complex alterations in brain function involving cognition, emotion, motivation, perception, sleep regulation, reward processing, and self-awareness. One of the greatest clinical challenges is that bipolar disorder often first appears as depression rather than mania. Many patients seek psychiatric care because of overwhelming hopelessness, fatigue, loss of interest, insomnia, suicidal thoughts, or emotional numbness. During these early episodes, there may be no obvious history of manic symptoms. As a result, bipolar disorder is frequently mistaken for major depressive disorder, sometimes for years before the first clear manic or hypomanic episode emerges. This delay has important consequences. Treatment strategies for bipolar depression differ significantly from those used for unipolar depression. When bipolar disorder remains unrecognized, symptoms may persist, relapse more frequently, or even become destabilized by inappropriate treatment. Understanding why mania can remain hidden therefore represents one of the most important questions in contemporary mood disorder research. To appreciate this phenomenon, it is first necessary to understand what psychiatrists mean by mania. Popular culture often portrays mania as extreme happiness. In reality, euphoria is only one possible presentation. Mania is fundamentally a disorder of mood regulation accompanied by pathological increases in energy, goal-directed behavior, cognitive speed, confidence, and physiological activation. The individual may sleep only a few hours while feeling fully rested. Ideas emerge rapidly. Speech accelerates. Attention shifts constantly between new possibilities. Ordinary limitations appear to disappear. At the same time, judgment frequently deteriorates. Risk-taking increases. Financial decisions become impulsive. Sexual behavior may become unusually uninhibited. Grandiose beliefs sometimes develop, ranging from exaggerated confidence to psychotic convictions involving extraordinary abilities or special missions. Importantly, mania is not always pleasant. Many episodes involve profound irritability rather than euphoria. The individual becomes impatient, argumentative, emotionally explosive, or intensely suspicious. Small frustrations provoke disproportionate anger. The enormous internal energy characteristic of mania may therefore manifest as agitation rather than excitement. This variability contributes substantially to diagnostic difficulty. Between severe depression and obvious mania lies hypomania. Hypomania shares many biological characteristics with mania but occurs at lower intensity. Individuals remain capable of functioning relatively well. Some even experience temporary improvements in productivity, creativity, sociability, or confidence. Because hypomania often feels subjectively positive, many patients do not consider it an illness. Instead, they describe it as finally feeling “normal” after prolonged depression. Consequently, clinicians may fail to identify previous hypomanic episodes unless detailed questioning is performed. This explains why bipolar disorder frequently remains hidden beneath repeated depressive episodes. Patients naturally focus on experiences that caused suffering. Periods of increased energy may be forgotten, minimized, or interpreted as healthy recovery. Family members sometimes recognize behavioral changes more readily than patients themselves. Mood disorders are increasingly understood through the concept of emotional regulation rather than isolated mood states. The healthy brain continuously maintains emotional balance despite changing circumstances. Neural systems regulating reward, motivation, circadian rhythms, stress responses, and executive control remain dynamically coordinated. Bipolar disorder appears to involve instability within these regulatory systems. Instead of maintaining equilibrium, mood regulation oscillates between pathological extremes. Depression and mania therefore represent different expressions of the same underlying dysregulation rather than independent illnesses. Circadian biology plays an especially important role. Sleep disturbances often precede manic episodes by days or weeks. Reduced need for sleep is not simply a symptom of mania. It may actively contribute to its development. The brain’s internal biological clock regulates numerous processes, including hormone secretion, body temperature, emotional regulation, cognitive performance, and neurotransmitter activity. Disruption of circadian rhythms appears capable of destabilizing mood regulation in genetically vulnerable individuals. This relationship explains why sleep deprivation can sometimes trigger manic episodes. It also explains why stabilizing sleep often becomes a central component of long-term treatment. Neurotransmitter systems contribute additional complexity. Earlier psychiatric models attempted to explain bipolar disorder through simple chemical imbalances involving serotonin, dopamine, or norepinephrine. Contemporary neuroscience recognizes that the disorder cannot be reduced to abnormalities in a single neurotransmitter. Instead, large-scale regulatory networks involving multiple neurotransmitter systems appear responsible. Dopaminergic signaling receives particular attention because dopamine influences reward anticipation, motivation, salience assignment, and goal-directed behavior. During mania, reward systems appear unusually sensitive. Ordinary opportunities generate extraordinary motivation. Novel ideas seem irresistibly important. The future appears filled with limitless possibility. Negative consequences receive insufficient attention. This imbalance contributes significantly to manic decision-making. One fascinating aspect of bipolar disorder concerns insight. During severe depression, individuals often recognize that something is profoundly wrong. During mania, awareness frequently decreases. The very brain systems responsible for evaluating judgment become altered. Consequently, patients may reject treatment despite obvious behavioral changes. From their perspective, they are functioning exceptionally well. Attempts by family members or clinicians to intervene may appear unnecessary or even threatening. Psychosis can occur during both manic and depressive episodes. In manic psychosis, grandiosity frequently dominates. Individuals may believe they possess extraordinary intelligence, unique spiritual importance, unlimited wealth, or special relationships with powerful figures. Ideas become increasingly disconnected from objective evidence. In depressive psychosis, delusions typically revolve around guilt, worthlessness, illness, punishment, or irreversible personal failure. These contrasting forms illustrate how mood profoundly influences the content of psychotic experience. Genetic research consistently demonstrates strong hereditary influences. Among major psychiatric disorders, bipolar disorder possesses one of the highest estimates of genetic contribution. However, inheritance remains probabilistic rather than deterministic. No single gene causes bipolar disorder. Instead, numerous genetic variations interact with developmental experiences, environmental stressors, sleep patterns, substance use, and biological vulnerability. This complex interaction explains why even identical twins are not always equally affected. Cognitive functioning also changes across mood episodes. During mania, thinking often becomes unusually rapid. Associations form quickly. Creativity may appear enhanced. Yet sustained attention deteriorates. Logical organization weakens. The individual generates enormous quantities of ideas while evaluating relatively few critically. This imbalance

Can the Brain Become Trapped in Fear?
Fear is one of the oldest and most evolutionarily conserved functions of the human nervous system. Long before the development of language, abstract reasoning, or self-awareness, survival depended upon the ability to detect danger rapidly and organize defensive behavior within fractions of a second. Every mammalian brain possesses sophisticated systems dedicated to recognizing potential threats, mobilizing physiological resources, and increasing the probability of survival. Under ordinary circumstances, these systems activate briefly, respond to immediate danger, and then gradually return to baseline once safety has been restored. Yet psychopathology reveals that this process does not always end when the threat disappears. In some individuals, the brain appears to remain organized around fear long after objective danger has passed. This raises one of the deepest questions in affective neuroscience and psychiatry: can the brain become permanently trapped inside its own survival state? At first glance, chronic fear appears to be simply an intensified version of normal anxiety. Contemporary neuroscience suggests something far more complex. Fear is not merely an emotion. It is an organizing principle capable of restructuring perception, memory, attention, decision-making, bodily awareness, and even personal identity. When fear becomes persistent, it does not simply coexist with other psychological processes. It gradually reorganizes them. To understand this transformation, it is necessary to abandon the popular misconception that fear originates from a single brain structure. Although the amygdala has become widely known as the “fear center,” modern neuroscience has demonstrated that no isolated region produces emotional experience independently. Fear emerges from interactions among distributed neural systems involving sensory processing, autonomic regulation, memory consolidation, executive control, interoception, hormonal signaling, and predictive computation. The amygdala contributes primarily to detecting biologically significant stimuli. It evaluates uncertainty rapidly. Its function is not to determine whether something is objectively dangerous but whether further attention should be allocated. This distinction is crucial. The amygdala responds to possibility rather than certainty. Evolution favored organisms that occasionally produced false alarms over those that failed to recognize genuine threats. Consequently, survival systems are intentionally biased toward caution. This adaptive bias becomes problematic when regulatory mechanisms begin interpreting ordinary uncertainty as continuous danger. Under normal circumstances, cortical regions gradually inhibit excessive alarm responses after evaluating additional evidence. The prefrontal cortex contributes substantially to this process by integrating contextual information, autobiographical knowledge, and long-term goals. Fear therefore reflects ongoing negotiation between rapid defensive systems and slower evaluative systems. Psychopathology emerges partly when this negotiation becomes chronically imbalanced. One of the most influential developments in contemporary neuroscience involves predictive coding models. According to these frameworks, perception is fundamentally anticipatory rather than reactive. The brain continuously generates predictions regarding incoming sensory information before external signals arrive. Incoming evidence is evaluated relative to these predictions. Fear profoundly influences this predictive architecture. An organism expecting danger allocates attention differently, interprets ambiguity differently, and encodes memory differently than an organism expecting safety. Over time, persistent fear gradually transforms prediction itself. Instead of predicting isolated threats, the nervous system begins predicting threat as the default condition. This transition represents one of the defining characteristics of chronic anxiety disorders. The external environment may remain objectively unchanged. The internal model organizing perception changes dramatically. Consequently, ordinary experiences acquire defensive significance. A crowded room becomes potential danger. Silence becomes suspicious. Physical sensations become possible illness. Neutral facial expressions become evidence of rejection. Importantly, these interpretations are not consciously fabricated. They emerge automatically because predictive systems continuously shape perception before conscious awareness fully develops. Memory undergoes equally profound transformation. The hippocampus ordinarily integrates experiences into coherent autobiographical narratives while simultaneously encoding contextual information distinguishing past from present. Fear alters these processes significantly. Stress hormones influence memory consolidation, increasing retention of threat-related information while reducing processing of contextual detail. From an evolutionary perspective, remembering danger possessed obvious survival value. However, excessive prioritization of threatening experiences gradually biases autobiographical memory itself. Individuals begin recalling danger more readily than safety. Negative experiences become cognitively accessible. Positive experiences require increasing effort to retrieve. Eventually, personal history appears organized primarily around threat. This transformation influences identity. Human beings understand themselves largely through remembered experience. If memory becomes selectively organized around fear, self-concept inevitably changes. Individuals begin viewing themselves as vulnerable, fragile, permanently endangered, or fundamentally incapable of safety. Identity shifts from describing who one is toward describing what one must avoid. Psychopathology therefore extends beyond emotional suffering into existential organization. The self gradually becomes structured around survival rather than development. Attention demonstrates similar reorganization. Ordinarily, attentional systems distribute cognitive resources flexibly according to changing environmental demands. Persistent fear dramatically narrows attentional priorities. Threat-related stimuli receive disproportionate processing. Neutral information becomes increasingly ignored. This phenomenon, known as attentional bias, has been repeatedly demonstrated across anxiety disorders. The implications extend beyond perception. Attention determines learning. Learning determines expectation. Expectation determines future attention. Fear therefore establishes recursive feedback loops. Each cycle strengthens subsequent cycles. Eventually, defensive attention begins maintaining itself independently of external circumstances. This self-perpetuating architecture explains why chronic anxiety frequently persists after objective danger has disappeared. Interoception introduces another essential dimension. The brain continuously monitors internal bodily states including heart rate, breathing, muscular tension, gastrointestinal activity, and hormonal fluctuations. These signals contribute substantially to emotional experience. Individuals rarely perceive bodily information directly. Instead, the brain interprets physiological patterns according to predictive models. Fear alters this interpretive process. Minor bodily sensations acquire catastrophic significance. Normal cardiac variations become evidence of impending death. Transient dizziness suggests neurological catastrophe. Ordinary respiratory changes indicate suffocation. The body itself becomes interpreted as a source of threat. Panic disorder illustrates this mechanism particularly clearly. Many patients begin fearing not external events but internal physiological sensations. The survival system turns inward. Ironically, attempts to monitor bodily danger often intensify precisely the physiological changes being feared. Hyperventilation increases dizziness. Muscular tension increases pain. Autonomic activation accelerates heart rate. The resulting sensations reinforce catastrophic predictions. Fear begins generating evidence supporting itself. Neuroendocrine systems contribute significantly to this persistence. Activation of the hypothalamic-pituitary-adrenal axis releases glucocorticoids facilitating adaptation during acute stress. Temporary activation enhances survival. Chronic activation produces