
Every human being experiences a persistent sense of “I.” Thoughts appear to belong to someone. Memories seem connected to a continuous identity. Decisions feel as though they are made by an internal self observing, evaluating, and directing experience. This inner self appears so obvious that most people rarely question its existence. Yet from a psychological and neuroscientific perspective, the nature of this self is surprisingly complex. The brain contains no single location where a unified “I” sits watching reality unfold. Instead, consciousness emerges from countless interacting processes involving perception, memory, emotion, prediction, language, and social cognition. This raises a profound question: Why does the mind create an inner self at all? To understand this, it is important first to recognize that survival requires continuity. An organism must distinguish itself from the environment in order to protect its body, obtain resources, avoid danger, and pursue goals. Without some form of self-representation, adaptive behavior would become nearly impossible. Even simple organisms demonstrate primitive forms of self-other distinction. However, human consciousness extends this process far beyond immediate physical boundaries. Humans do not merely experience a physical body. They experience a psychological identity. This identity stretches across years, sometimes decades, linking childhood memories to future plans through a single narrative perspective. The remarkable aspect of this continuity is that it often feels permanent despite constant change. Cells die and regenerate. Beliefs evolve. Relationships change. Goals shift. Memories transform. Yet the subjective feeling of being the same person often persists. Psychologically, this continuity serves an important function. Without it, experiences would remain disconnected fragments. Memory would lose coherence. Planning would become difficult. Responsibility would become meaningless. The self acts as an organizing principle that binds diverse experiences together. In many ways, the self functions like a story. This comparison is not intended to suggest that the self is imaginary. Rather, it highlights that identity depends heavily upon narrative organization. People continuously construct explanations regarding who they are. These explanations include personal history, values, relationships, strengths, weaknesses, hopes, fears, and aspirations. The resulting narrative creates stability within an otherwise changing psychological landscape. Importantly, this narrative is constantly updated. When new experiences occur, they must be integrated into existing identity structures. Sometimes this integration is easy. Sometimes it creates conflict. For example, imagine a person who sees themselves as honest but later discovers evidence of behavior contradicting that self-image. Psychological discomfort emerges because the identity narrative has been challenged. The mind must either revise the narrative or reinterpret the experience. This process illustrates that the self is dynamic rather than fixed. Memory plays a central role here. Autobiographical memory allows individuals to perceive themselves across time. Without memory, continuity of identity weakens dramatically. Certain neurological conditions demonstrate this clearly. Individuals with severe memory impairments often struggle maintaining stable self-concepts because experiences cannot be integrated effectively into long-term narrative structures. However, memory alone cannot explain the self. After all, memory itself is reconstructive. As discussed previously, memories change over time. They are influenced by emotion, interpretation, and present identity. This creates a fascinating feedback loop. The self shapes memory. Memory shapes the self. Each continuously influences the other. Consequently, identity is not simply discovered through memory but actively constructed through ongoing interpretation. Social interaction contributes enormously to this construction. Human beings evolved within intensely relational environments. Survival depended upon cooperation, communication, and group membership. As a result, much of the self develops through interaction with others. Children learn who they are partly through how caregivers respond to them. Praise, criticism, affection, neglect, and expectation all influence identity formation. Over time, external perspectives become internalized. People begin carrying imagined social audiences within their own minds. This internal audience influences behavior even when nobody else is physically present. For example, individuals often evaluate themselves through standards learned from parents, peers, teachers, or cultural norms. The self therefore contains social elements from the very beginning. In a sense, identity is partly relational memory made internal. Language further transforms selfhood. Human beings possess the ability to describe themselves symbolically. Thoughts can be converted into narratives. Emotions can be labeled. Experiences can be categorized. Language allows the mind to reflect upon itself recursively. A person can think about thinking. Observe observation. Question identity itself. This recursive capacity creates extraordinary psychological complexity. The self becomes both subject and object simultaneously. One part of consciousness experiences life. Another part evaluates that experience. Another interprets it. Another imagines future consequences. The result is a layered psychological structure rather than a single unified entity. Neuroscience supports this view. Different aspects of selfhood involve different neural systems. Body awareness, autobiographical memory, emotional processing, social cognition, and future planning each rely upon partially distinct networks. Yet consciousness integrates these processes into a coherent subjective experience. This integration creates the impression of a singular self. Importantly, the feeling of unity may itself be a construction. The brain continuously combines diverse information streams into a stable representation because coherence improves adaptive functioning. Without such integration, consciousness would become fragmented. Certain psychological conditions reveal what happens when integration weakens. Dissociation provides one example. During dissociative states, individuals may feel detached from themselves, their bodies, or their surroundings. The normally unified sense of identity becomes disrupted. People often describe feeling like observers of their own lives rather than active participants. These experiences demonstrate that selfhood is not guaranteed. It requires ongoing psychological organization. Depersonalization offers another example. Individuals experiencing depersonalization frequently report that they still possess memories, thoughts, and awareness, yet the feeling of being a unified self becomes strangely diminished. The world may appear normal, but the sense of ownership over experience weakens. Such cases reveal how complex and fragile selfhood can be. Dreams provide additional insight. During dreams, identity often changes dramatically. People may become different versions of themselves, occupy unfamiliar roles, or accept bizarre circumstances without questioning them. Yet a sense of self usually remains present in some form. This suggests that selfhood is highly flexible. The mind continuously reconstructs identity according to context. Meditation traditions have explored these
Why Does Consciousness Need Meaning?
Among the countless psychological needs that shape human experience, the search for meaning may be one of the most powerful and least understood. Human beings do not merely seek pleasure, safety, food, status, or social connection. They also seek explanation. People want to know why events happen, why suffering exists, why relationships end, why death occurs, why they themselves exist, and whether their experiences possess significance beyond immediate circumstances. When meaning collapses, emotional stability often deteriorates even when material survival remains secure. This suggests that meaning is not a luxury added onto consciousness but a fundamental psychological function. The question is why. Why does consciousness need meaning at all? To answer this, it is necessary first to understand that human beings possess a unique cognitive capacity rarely seen elsewhere in nature: the ability to perceive themselves across time. The human mind remembers the past, imagines the future, evaluates the present, and continuously compares these temporal perspectives. This ability provides extraordinary advantages. It allows planning, learning, cooperation, and complex culture. Yet it also creates psychological burdens. Unlike most animals, humans recognize mortality. They understand that relationships end, bodies age, opportunities disappear, and life itself possesses limits. Consciousness therefore confronts uncertainty, loss, and impermanence constantly. Meaning functions partly as a response to this awareness. Without meaning, experiences become isolated events lacking narrative connection. Suffering feels random. Success feels temporary. Relationships appear fragile. Mortality becomes psychologically overwhelming. Meaning organizes experience into a coherent structure. From a psychological perspective, coherence is essential because the brain evolved to identify patterns. Randomness creates uncertainty, and uncertainty activates threat systems. Consequently, the mind continuously searches for explanations capable of transforming confusion into understanding. Importantly, meaning does not require objective truth to provide psychological stability. A belief system may reduce distress because it organizes experience coherently, even if certain aspects of that system cannot be empirically verified. This explains why meaning-making appears universally across cultures. Religions, philosophies, myths, political ideologies, scientific frameworks, and personal narratives all attempt answering fundamental questions regarding existence. Although their conclusions differ dramatically, they serve similar psychological functions: they reduce ambiguity and organize experience. The search for meaning becomes especially intense during suffering. When painful events occur, individuals rarely ask only “What happened?” They ask “Why did this happen?” This distinction is crucial. The factual description of an event often fails to satisfy consciousness emotionally. People seek significance because emotional systems require contextual integration. Pain without meaning becomes psychologically difficult to tolerate. Consider grief. The death of a loved one creates more than emotional loss. It often disrupts the narrative structure through which individuals understood themselves and their future. The bereaved person must reconstruct meaning because the previous psychological world no longer exists. This reconstruction process explains why grief frequently involves existential reflection. Individuals question identity, purpose, mortality, and relationship significance because meaning structures have been destabilized. Trauma reveals similar dynamics. Traumatic experiences often shatter assumptions regarding safety, fairness, predictability, and control. Recovery therefore involves more than symptom reduction. It frequently requires rebuilding meaning systems capable of integrating overwhelming experiences. People commonly ask: Why did this happen to me? What does this experience mean? Who am I now? These questions emerge because consciousness seeks narrative coherence even under devastating circumstances. Memory plays an important role here. Human beings do not remember experiences simply as isolated data. Memories become embedded within broader stories regarding identity and life trajectory. Meaning determines which memories receive emphasis, how they are interpreted, and how they influence future behavior. Two individuals may experience similar events yet construct entirely different meanings. One person interprets hardship as evidence of personal failure. Another interprets the same hardship as evidence of resilience and growth. The emotional consequences differ dramatically because meaning alters psychological reality. Importantly, meaning is not merely intellectual. Many people assume meaning exists primarily in philosophical reflection or religious belief. In reality, meaning operates continuously at emotional and perceptual levels. Relationships provide meaning. Work provides meaning. Creativity provides meaning. Parenthood provides meaning. Community provides meaning. Even small daily routines often contribute meaning by creating continuity and structure. When these sources disappear suddenly, individuals frequently experience profound disorientation because meaning systems have been disrupted. Loneliness demonstrates this clearly. Human beings evolved within social groups where identity and purpose emerged relationally. Isolation therefore threatens not only emotional comfort but existential orientation itself. Lonely individuals often report feelings of emptiness extending beyond sadness. They struggle with questions regarding significance, belonging, and purpose because social connection contributes heavily to meaning construction. Neuroscience provides additional insight. The brain continuously attempts integrating information into coherent models. Predictive systems organize perception, memory, emotion, and expectation into narratives that guide behavior. Meaning may therefore represent a large-scale expression of predictive organization. Without meaning, experiences remain fragmented. With meaning, experiences become integrated. This integration reduces cognitive load because the brain no longer processes every event independently. Instead, events become components within larger explanatory structures. The desire for meaning is therefore partly a desire for psychological efficiency. Uncertainty complicates this process significantly. As discussed previously, the brain dislikes ambiguity because uncertainty undermines prediction. Meaning reduces uncertainty by providing explanatory frameworks. However, this creates an important vulnerability. People sometimes accept inaccurate explanations because explanation itself feels emotionally preferable to uncertainty. Conspiracy theories, extreme ideologies, and rigid belief systems often become attractive during periods of social instability because they provide certainty and narrative structure. Psychologically, a coherent explanation may feel safer than admitting complexity and ambiguity. This tendency reveals that meaning can both stabilize and distort perception. The same cognitive mechanisms supporting resilience and purpose may also reinforce dogmatism when flexibility disappears. Existential psychology explores these issues deeply. According to existential thinkers, humans confront four fundamental realities: mortality, freedom, isolation, and uncertainty. Meaning emerges partly as a response to these realities. Mortality creates urgency. Freedom creates responsibility. Isolation creates longing for connection. Uncertainty creates desire for understanding. Meaning helps organize these tensions into psychologically survivable forms. Importantly, meaning is not always discovered. Often it is created. This distinction matters because many individuals search
Why Does The Brain Fear Uncertainty?
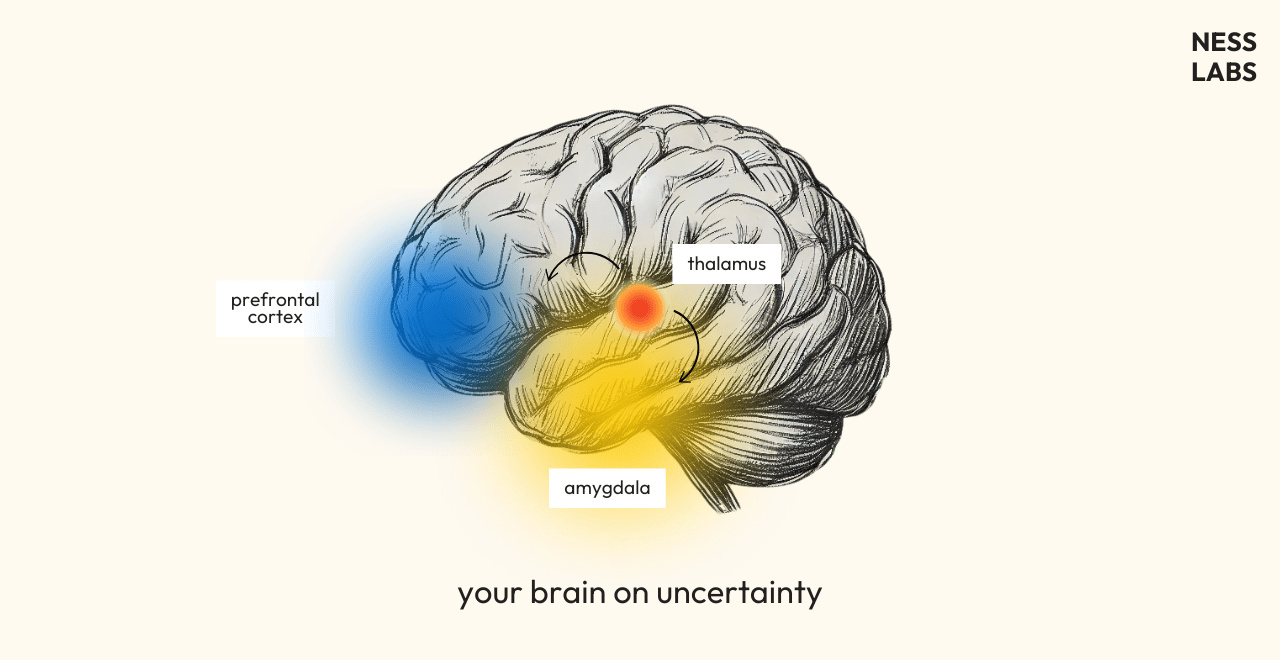
Among all psychological experiences capable of destabilizing human consciousness, uncertainty occupies a uniquely powerful position. People often tolerate pain, grief, hardship, or even danger more effectively than ambiguity regarding what may happen next. Uncertainty amplifies anxiety, intensifies obsessive thinking, distorts perception, and alters emotional regulation in ways that frequently exceed the distress caused by confirmed negative outcomes themselves. Individuals awaiting medical results, relationship decisions, financial collapse, social rejection, or existential answers commonly report that the unknown becomes psychologically unbearable long before reality arrives. This raises a profound neuropsychological question: why does the brain fear uncertainty so intensely, and why does ambiguity itself become emotionally threatening even in the absence of immediate danger? To understand this phenomenon, it is first necessary to recognize that the human nervous system evolved fundamentally as a predictive organ. The brain’s primary task is not merely reacting to the present moment but anticipating future conditions in order to guide survival behavior efficiently. Prediction allows organisms to conserve energy, avoid danger, maintain social stability, and prepare adaptive responses before threats fully emerge. Certainty therefore provides neurological efficiency. When the environment becomes predictable, the nervous system reduces metabolic and emotional expenditure because future outcomes can be anticipated with relative confidence. Routine, familiarity, and stable expectation allow attentional systems to relax partially, freeing cognitive resources for exploration, social interaction, and long-term planning. Uncertainty disrupts this predictive stability completely. Under ambiguous conditions, the brain loses confidence regarding what actions will preserve safety or emotional equilibrium. Predictive systems become hyperactive because multiple possible outcomes must be monitored simultaneously. The nervous system therefore enters a state of heightened vigilance designed to detect relevant information rapidly. Importantly, this vigilance is emotionally costly. The uncertain brain continuously scans for clues, patterns, and signs capable of reducing ambiguity. Thoughts loop repeatedly around unresolved possibilities because prediction systems cannot achieve closure. The result is rumination, compulsive checking, catastrophic imagination, and emotional exhaustion. From an evolutionary perspective, this response makes sense. In ancestral environments, uncertainty often signaled hidden danger. Unclear sounds in darkness, unpredictable weather, unfamiliar strangers, or ambiguous social dynamics carried genuine survival consequences. Organisms that remained highly sensitive to uncertainty therefore possessed adaptive advantages because ambiguity itself frequently preceded threat. Consequently, the nervous system evolved to treat uncertainty not as neutral absence of information but as a potential indicator of danger. This explains why the brain often prefers negative certainty over unresolved ambiguity. A confirmed threat allows organized response. Uncertainty, by contrast, prevents resolution because the nervous system cannot determine whether defensive action is necessary or what form it should take. The emotional tension produced by this unresolved state becomes psychologically aversive. Anxiety emerges directly from this predictive instability. Unlike fear, which typically responds to identifiable threat, anxiety concerns uncertain future possibilities. The anxious mind attempts compensating for ambiguity through hyperanalysis, overpreparation, avoidance, reassurance-seeking, or catastrophic simulation. These behaviors represent attempts to restore predictive control. Catastrophic thinking is particularly important here. Many individuals assume anxiety exaggerates negativity irrationally, yet catastrophizing often functions psychologically as defensive prediction. The mind imagines worst-case scenarios because preparing emotionally for disaster feels safer than remaining uncertain. Paradoxically, certainty about catastrophe may feel temporarily more tolerable than unresolved ambiguity because at least the future becomes conceptually organized. Obsessive-compulsive behaviors reveal these mechanisms dramatically. Compulsions such as checking, counting, reassurance-seeking, or ritual repetition often emerge from inability to tolerate uncertainty rather than from the feared outcome itself. The compulsive act temporarily reduces ambiguity, creating brief relief before uncertainty inevitably returns. The cycle persists because the brain learns associating ritualized behavior with predictive stabilization. Social uncertainty affects humans especially strongly because survival historically depended upon group belonging. Ambiguous social signals—unclear facial expressions, delayed responses, inconsistent affection, uncertain status—activate threat-processing systems intensely. Individuals experiencing attachment insecurity frequently become hypervigilant toward relational ambiguity. A short message lacking emotional clarity may trigger disproportionate distress because uncertainty regarding connection activates deep predictive fear surrounding abandonment or rejection. Importantly, the emotional intensity often reflects not objective danger but the nervous system’s inability to resolve ambiguous relational signals confidently. Trauma intensifies intolerance of uncertainty profoundly. Traumatic experiences teach the nervous system that unexpected events may produce overwhelming helplessness or danger. After trauma, predictive systems become organized around preventing surprise itself. Hypervigilance therefore emerges partly as an attempt to eliminate uncertainty through continuous monitoring. Traumatized individuals often struggle intensely with unpredictability because uncertainty reactivates emotional memories associated with loss of control. Even minor ambiguity may trigger exaggerated autonomic arousal because the nervous system interprets unpredictability as inherently unsafe. Children illustrate the developmental roots of these processes clearly. Young children rely heavily upon routine and predictable caregiving because stable patterns support emotional regulation and attachment security. Unpredictable environments increase anxiety because the developing nervous system lacks sufficient cognitive flexibility to tolerate ambiguity comfortably. Over time, healthy development strengthens uncertainty tolerance gradually through repeated experiences demonstrating that unpredictability does not always result in catastrophe. However, chronic instability during development may produce persistent hypersensitivity to uncertainty throughout adulthood. Neurobiologically, uncertainty strongly activates emotional and attentional systems involved in threat anticipation. The brain responds not only to actual danger but to prediction error—the mismatch between expected and uncertain outcomes. Under ambiguous conditions, predictive models lose reliability, increasing cognitive and emotional effort dramatically. Stress hormones rise because the nervous system prepares for multiple possible scenarios simultaneously. This state is metabolically expensive and psychologically exhausting. Importantly, uncertainty amplifies imagination. When concrete information is absent, the mind fills gaps using memory, fear, expectation, and symbolic association. The brain continuously generates possible futures in attempts reducing unpredictability. Yet because emotionally salient possibilities receive attentional priority, negative scenarios often dominate awareness disproportionately. This explains why uncertain situations frequently feel worse psychologically than confirmed outcomes. Imagination produces endless hypothetical threats unconstrained by objective limitation. Silence intensifies uncertainty similarly. In quiet or ambiguous environments, predictive systems search aggressively for hidden meaning because reduced sensory information weakens environmental certainty. Minor sounds acquire exaggerated significance while the absence of explanation itself becomes emotionally threatening. This mechanism contributes to experiences of paranoia, haunting
Why Does Fear Distort Perception?
Fear is often described emotionally, yet its effects extend far beyond feeling alone. Under fear, the world itself changes psychologically. Time slows or accelerates unpredictably, sounds become sharper, shadows appear threatening, faces seem unreadable, distances distort, and ordinary environments acquire emotional hostility. Individuals experiencing intense fear frequently report certainty about dangers later revealed to be exaggerated, misinterpreted, or entirely absent. This raises a fundamental psychological and neurobiological question: why does fear distort perception so profoundly, and what mechanisms transform emotional threat into altered reality itself? To answer this question, it is necessary first to recognize that perception is never neutral observation. Human beings do not passively receive reality through the senses. Instead, the brain continuously constructs perception through predictive interpretation. Sensory input provides incomplete information, which cognitive systems organize into coherent experience using memory, expectation, emotional significance, and survival priorities. Fear radically alters this interpretive process because survival becomes the dominant organizational principle. From an evolutionary perspective, fear exists not to produce objective understanding but to maximize protection under uncertainty. The nervous system evolved in environments where failing to detect danger could result in death, while overestimating threat often carried comparatively smaller costs. Consequently, human perception became biased toward false-positive threat detection. This means the frightened brain intentionally sacrifices accuracy for survival probability. Under fear, attentional systems narrow dramatically toward potentially threatening stimuli. This process, often called attentional bias, allows rapid focus on environmental danger while suppressing less immediately relevant information. In survival contexts such narrowing can be adaptive because it prioritizes reaction speed over reflective analysis. However, attentional narrowing also distorts perception by reducing contextual integration. Individuals become hyperfocused on isolated cues interpreted through fear while ignoring contradictory evidence that might otherwise moderate emotional conclusions. For example, a harmless sound at night may immediately acquire threatening significance because fear directs attention toward ambiguity itself. The nervous system assumes danger first and evaluates alternatives later. Physiologically, fear activates extensive autonomic changes involving the sympathetic nervous system. Heart rate increases, muscle tension rises, breathing alters, pupils dilate, and stress hormones flood the body. These changes prepare rapid defensive action but simultaneously transform subjective experience. Time perception becomes particularly unstable during fear. Many individuals report that frightening moments feel unusually prolonged. This phenomenon likely emerges because heightened arousal increases attentional density. The brain encodes more sensory information per subjective moment during threat states, creating retrospective impressions that events lasted longer than they objectively did. Yet fear may also produce the opposite effect. In overwhelming situations individuals sometimes experience temporal fragmentation or abrupt memory gaps because extreme stress disrupts coherent encoding. Time may feel simultaneously slowed and unreal. This instability reveals that temporal experience is psychologically constructed rather than mechanically fixed. Visual perception changes profoundly under fear as well. Threat-related stimuli become perceptually prioritized, while neutral information fades into the background. Ambiguous shapes are more likely interpreted as dangerous, facial expressions appear more hostile, and environmental uncertainty becomes emotionally magnified. Importantly, these distortions occur automatically rather than consciously. Fear changes perception before deliberate reasoning begins. One powerful mechanism underlying these effects involves predictive processing. The brain continuously generates expectations about the environment based on prior experience and emotional context. Sensory information is then interpreted relative to these predictions rather than processed objectively from scratch. Fear shifts predictive models toward threat anticipation. Once the nervous system expects danger, ambiguous stimuli become integrated according to fear-consistent interpretation. A shadow resembles a figure, silence feels occupied, distant footsteps imply pursuit, and uncertain social interactions appear rejecting or hostile. This predictive bias explains why fear can feel self-confirming. The frightened mind perceives evidence supporting its own expectations because perception itself becomes organized around anticipated threat. Trauma intensifies these mechanisms dramatically. Traumatic experiences reorganize predictive systems around survival models developed during overwhelming danger. After trauma, the nervous system may continue interpreting ordinary environments through frameworks optimized for past threat rather than present safety. Hypervigilance emerges from this persistent predictive adaptation. Traumatized individuals often scan environments continuously for signs of danger, even when objective threat is minimal. Because attention remains organized around detection, ambiguous stimuli repeatedly activate fear responses. Importantly, hypervigilance is not irrational in its original context. It represents survival learning extended beyond the circumstances that initially required it. The nervous system prefers maintaining readiness rather than risking vulnerability. Fear also alters auditory perception significantly. Under threat, unexpected sounds become amplified emotionally and perceptually. Silence itself may become psychologically threatening because ambiguity increases predictive uncertainty. The frightened brain fills informational gaps with imagined possibilities consistent with danger anticipation. This explains why isolated or dark environments often intensify anxiety. Reduced sensory certainty increases reliance upon internally generated prediction, and fearful prediction naturally prioritizes hidden threat. Social perception becomes distorted under fear as well. Human beings evolved within intensely social environments where group rejection or hostility historically carried survival consequences. Consequently, fear strongly affects interpretation of facial expressions, tone of voice, and interpersonal behavior. Anxious individuals frequently overestimate social threat, perceiving criticism, judgment, or rejection where ambiguity exists. Neutral expressions may appear hostile because fear biases interpretation toward negative outcomes. Social anxiety therefore involves not merely excessive emotion but altered social perception itself. Memory interacts closely with these distortions. Fear enhances encoding of emotionally salient threat-related details while impairing broader contextual integration. Later recall may therefore emphasize danger disproportionately relative to the full situation. Repeated fearful remembering further strengthens these patterns through reconsolidation. Each fearful recollection reinforces emotional associations, making future threat perception increasingly automatic. The world gradually appears more dangerous because memory continuously reorganizes perception around prior fear. Dissociation represents another important response to overwhelming fear. When threat exceeds coping capacity, consciousness may partially detach from direct experience. Individuals report unreality, emotional numbness, altered bodily perception, or dreamlike surroundings. Paradoxically, dissociation functions protectively by reducing unbearable emotional intensity. Yet because perception becomes fragmented, environments may feel strange, artificial, or threatening afterward. Fear therefore destabilizes not only emotional regulation but reality integration itself. Children illustrate fear-based perception particularly clearly. Young children frequently perceive monsters, hidden presences, or threatening figures
Why Do Memories Change Over Time?
Human beings often imagine memory as a form of internal recording—a psychological archive preserving experiences in stable form across time. This assumption feels intuitively convincing because memories frequently carry vivid sensory detail and emotional certainty. People speak of “replaying” childhood moments, “retrieving” forgotten experiences, or “reliving” emotional events as though the past exists intact somewhere within the mind awaiting access. Yet cognitive neuroscience demonstrates something far more psychologically unsettling: memories are not preserved unchanged. Instead, every act of remembering partially reconstructs and alters the memory itself. The past is therefore not simply stored within consciousness but continuously rewritten by emotion, interpretation, expectation, and present identity. This raises a profound psychological question: why do memories change over time, and what does this instability reveal about the nature of consciousness and personal reality? To understand memory transformation, it is first necessary to reject the metaphor of memory as passive storage. Human memory evolved not primarily to preserve objective history but to support survival, prediction, emotional regulation, and identity continuity. From an evolutionary perspective, perfectly accurate recall is often less important than flexible adaptation. Consequently, memory functions reconstructively rather than reproductively. When individuals remember an experience, they do not retrieve a complete preserved event. Instead, the brain reconstructs the experience dynamically using fragments of sensory information, emotional associations, narrative expectations, and present cognitive context. This reconstruction process explains why memories are inherently unstable. Each time a memory is recalled, it temporarily re-enters a malleable state known as reconsolidation. During reconsolidation, the memory becomes vulnerable to modification before being stored again. New emotions, interpretations, beliefs, and contextual information may therefore become integrated into the remembered event itself. Importantly, individuals rarely perceive this alteration consciously. The updated memory still feels authentic because subjective certainty depends more upon emotional coherence than objective accuracy. The mind experiences reconstructed memories as direct access to the past even while continuously reshaping them. Emotion plays a particularly powerful role in this process. Emotional intensity strengthens memory encoding initially because emotionally significant events carry adaptive importance. However, emotion also distorts perception and recall selectively. During emotionally charged situations, attention narrows toward specific details while peripheral information may disappear entirely. For example, individuals experiencing fear often remember threat-related elements vividly while misremembering contextual details surrounding them. Over time, repeated emotional reflection may further exaggerate or simplify certain aspects of the event according to the emotional meaning attached to it. Trauma illustrates these dynamics dramatically. Contrary to popular assumptions, traumatic memories are not always perfectly preserved. Some traumatic experiences remain fragmented, sensory-based, or disorganized precisely because overwhelming emotional arousal disrupts ordinary encoding and integration processes. At the same time, repeated rumination about trauma may reinforce particular interpretations while suppressing alternative contextual understanding. The traumatic memory gradually becomes organized around dominant emotional themes such as helplessness, betrayal, shame, or danger. As a result, the remembered event may shift psychologically over years even when the individual believes they are recalling it accurately. The emotional truth remains real, yet narrative structure and sensory details evolve according to ongoing psychological needs and fears. Identity formation strongly influences memory transformation as well. Human beings continuously construct narratives explaining who they are, how they became that person, and what their experiences mean. Memories are reorganized constantly to maintain coherence within these evolving self-narratives. This means the present self partially edits the remembered past. Events inconsistent with current identity may fade, while experiences supporting existing beliefs become more accessible and emotionally convincing. Individuals therefore remember not only what happened but what feels psychologically meaningful in relation to current self-understanding. For example, someone who now views childhood as lonely may increasingly recall memories consistent with isolation while overlooking contradictory experiences of connection or joy. Conversely, individuals idealizing the past may reconstruct earlier life periods as more stable or meaningful than they actually felt at the time. Importantly, this process is not deliberate dishonesty. Memory naturally organizes itself around emotional and narrative coherence because coherence stabilizes identity psychologically. Social influence also reshapes memory continuously. Conversations, family narratives, photographs, media exposure, and repeated retelling alter how experiences are encoded retrospectively. Over time, externally supplied interpretations may become integrated into personal memory so completely that individuals cannot distinguish original perception from later reconstruction. False memory research demonstrates this vulnerability clearly. Under suggestive conditions, people may develop highly vivid memories for events that never occurred or significantly distort genuine experiences. These memories often feel emotionally authentic because the mechanisms generating familiarity and confidence are psychologically separate from factual verification. The existence of false memory does not imply memory is useless or entirely unreliable. Rather, it reveals that memory prioritizes plausibility, emotional meaning, and narrative integration over perfect historical accuracy. Prediction systems contribute importantly here as well. The brain continuously uses past experience to anticipate future possibilities. Memories therefore function partly as predictive models rather than static records. Events are remembered according to how they help organize expectations regarding safety, relationships, identity, and environment. This predictive role explains why memories often become simplified into emotionally meaningful patterns. The mind extracts general lessons and emotional associations from complex experiences to guide future behavior efficiently. Nuance may therefore disappear over time while emotionally relevant themes intensify. Childhood memory demonstrates these principles particularly clearly. Many early memories are reconstructed heavily through family stories, photographs, emotional atmosphere, and later interpretation rather than preserved direct experience. Yet these reconstructed memories still influence identity profoundly because psychological impact depends more upon narrative integration than objective precision. The phenomenon of nostalgia reveals another important dimension of memory alteration. Nostalgia often transforms past experiences into emotionally idealized versions emphasizing warmth, coherence, and meaning. Difficulties fade while emotionally comforting elements become amplified. Psychologically, nostalgia serves regulatory functions during uncertainty or distress by restoring continuity and emotional grounding. However, nostalgic memory frequently sacrifices factual complexity for emotional reassurance. The remembered past becomes symbolically meaningful rather than historically precise. Time itself changes memory through repeated reinterpretation. Experiences acquire new meanings as individuals age because current perspective reshapes understanding of previous events. A painful breakup, parental conflict,
Why Does Silence Become Psychologically Loud?
Silence is often imagined as the absence of experience, yet psychologically it rarely functions as emptiness. In many situations silence becomes intensely present, emotionally charged, and even physically overwhelming. Individuals isolated in quiet environments frequently report heightened anxiety, intrusive thoughts, distorted time perception, amplified bodily awareness, and sensations of unreality or hidden presence. Long periods without external stimulation may transform ordinary consciousness itself, making the mind feel louder, stranger, and increasingly difficult to regulate. This paradox raises an important psychological and neurocognitive question: why does silence become psychologically loud, and why does the absence of external noise often intensify internal experience rather than diminish it? To understand this phenomenon, it is necessary first to recognize that the human nervous system evolved within environments rich in continuous sensory input. Wind, movement, speech, animal sounds, environmental rhythms, and social interaction historically surrounded human perception almost constantly. The brain therefore developed not merely to process stimuli but to predict their continuity. Silence interrupts these predictive expectations. Importantly, the brain is not passive during quiet conditions. When external stimulation decreases, internally generated activity becomes more perceptually dominant. Thoughts, memories, bodily sensations, emotional states, and predictive simulations emerge into awareness with increased intensity because fewer external signals compete for attentional resources. In this sense, silence does not remove experience. It redistributes attention inward. One of the most immediate effects of silence involves heightened interoception—the perception of internal bodily states. In quiet environments individuals suddenly become aware of heartbeat, breathing, muscle tension, swallowing, pulse rhythms, and subtle visceral sensations ordinarily ignored during active engagement with external reality. This heightened bodily awareness can become emotionally destabilizing because internal sensations are inherently ambiguous. A slight change in heartbeat may be interpreted as anxiety, illness, danger, or existential vulnerability depending upon context and emotional state. Once attention fixates on bodily signals, feedback loops emerge. Anxiety increases physiological arousal, which intensifies bodily sensation further, amplifying awareness recursively. Silence therefore often magnifies emotional states already present beneath conscious distraction. Modern life provides continuous sensory and informational stimulation partly because distraction regulates psychological discomfort. Noise, conversation, digital media, work routines, and environmental activity occupy attentional systems externally, reducing direct confrontation with unresolved internal material. When silence removes these distractions, suppressed thoughts frequently return with surprising force. Regrets, fears, unresolved grief, intrusive memories, existential concerns, and identity conflicts become more difficult to avoid because attentional escape routes narrow significantly. This process explains why some individuals experience quiet environments as calming while others experience them as threatening. Silence itself is not emotionally neutral; its psychological meaning depends largely upon what emerges internally once distraction disappears. Trauma profoundly alters responses to silence. Traumatized nervous systems remain organized around heightened threat anticipation. In quiet environments, the absence of predictable sensory information may actually increase vigilance rather than relaxation. Ambiguity becomes threatening because the nervous system expects hidden danger. Consequently, silence may feel psychologically unsafe. Minor environmental sounds become exaggerated in significance, while the absence of reassuring social or sensory input intensifies anticipatory anxiety. Some individuals therefore maintain constant background noise unconsciously to regulate hypervigilance and reduce exposure to intrusive internal states. Loneliness intensifies these effects further. Human beings evolved within deeply social environments where interpersonal interaction continuously regulated emotion, attention, and physiological state. Silence combined with isolation removes important regulatory feedback mechanisms provided by other people. Without external relational anchors, self-referential cognition becomes increasingly dominant. Individuals begin monitoring thoughts, emotions, and perceptions more intensely. Over time this can produce rumination, derealization, dissociation, or exaggerated self-consciousness. Rumination is especially important here. In silence, repetitive thought loops often become amplified because there are fewer competing stimuli interrupting them. The mind revisits unresolved problems repeatedly in attempts to achieve cognitive closure. However, chronic rumination rarely produces genuine resolution. Instead, it strengthens emotional salience surrounding distressing themes. The result is the subjective impression that thoughts themselves have become louder. Neuroscientifically, this shift relates partly to activity within the default mode network—a system associated with self-referential thinking, autobiographical reflection, future simulation, and internal narrative generation. When external task engagement decreases, default mode activity becomes more prominent. This internally oriented network plays crucial roles in identity construction and meaning-making. Yet excessive or dysregulated default mode activity is also associated with anxiety, depression, intrusive thought, and dissociation. Silence therefore increases exposure to the mind’s spontaneous narrative production. Importantly, spontaneous cognition is not random. The brain continuously simulates possibilities, reconstructs memories, anticipates future scenarios, and organizes emotional meaning automatically. Silence merely makes these ongoing processes more noticeable. Time perception changes significantly under prolonged quiet as well. External stimulation normally structures temporal awareness through events, interactions, and sensory transitions. In silence, these temporal markers diminish. Time may therefore feel slowed, suspended, or strangely expanded. This alteration can become psychologically unsettling because ordinary consciousness depends heavily upon stable temporal orientation. Without external anchors, subjective time becomes increasingly dependent upon internal emotional states. Anxiety often lengthens perceived duration, while monotony dissolves temporal boundaries altogether. Sensory deprivation research demonstrates these effects dramatically. Individuals placed in environments with reduced sensory input frequently begin experiencing cognitive distortions, heightened suggestibility, altered body perception, and hallucination-like phenomena after extended periods. These experiences emerge because predictive systems require continuous input to stabilize perception. When external information decreases substantially, the brain compensates by increasing internally generated imagery and interpretation. Hallucinations in sensory deprivation are therefore not evidence of madness but expressions of predictive cognition deprived of environmental calibration. Silence can also amplify agency detection systems. Humans evolved to remain highly sensitive to hidden presence under uncertain conditions. In quiet environments, ambiguous sounds or subtle sensory changes acquire disproportionate salience because the brain actively searches for explanation. This mechanism explains why silence often feels “occupied” rather than empty. Individuals alone in silent houses, forests, or unfamiliar environments frequently report sensations of observation or invisible presence. These experiences emerge because predictive threat systems interpret ambiguity conservatively, preferring false-positive detection over missed danger. Importantly, such sensations feel profoundly real despite lacking external confirmation. The emotional certainty arises from autonomic activation and attentional narrowing rather than objective
Why Does The Mind Create Alternate Realities?
Human consciousness possesses a remarkable capacity to generate realities that exist partially independent of immediate external conditions. Fantasies, intrusive thoughts, dissociative states, immersive memories, paranoid interpretations, lucid dreams, imagined conversations, future simulations, and emotionally charged internal narratives all demonstrate that the mind continuously constructs experiential worlds beyond direct sensory reality. Under ordinary conditions these internally generated realities remain flexible and clearly distinguishable from external events. Yet under stress, trauma, isolation, emotional overload, or neurological instability, the boundary between constructed reality and shared reality may weaken significantly. This raises a fundamental psychological question: why does the mind create alternate realities at all, and what adaptive or pathological functions do these internally constructed worlds serve? To answer this question, it is necessary first to abandon the assumption that consciousness evolved primarily to perceive objective reality accurately. From an evolutionary perspective, the brain evolved not to produce philosophical truth but to maximize survival, prediction, emotional regulation, and behavioral adaptation. Reality perception therefore functions pragmatically rather than neutrally. The mind continuously edits, simplifies, predicts, and reorganizes information according to biological and psychological priorities. What humans experience as “reality” is already a constructed interpretation rather than direct access to the external world. Sensory systems receive incomplete information, which predictive cognitive systems transform into coherent experience through expectation, memory, and contextual inference. Consciousness itself is therefore fundamentally generative. Alternate realities emerge naturally from this generative architecture. One of the primary functions of internally constructed realities involves predictive simulation. Human beings possess the extraordinary ability to imagine futures before they occur. This capacity allows rehearsal of danger, planning of social interactions, anticipation of consequences, and preparation for uncertainty. Daydreaming represents one common form of predictive simulation. While often dismissed as distraction, daydreaming allows the mind to explore hypothetical situations emotionally and cognitively without direct real-world risk. Individuals rehearse conversations, conflicts, ambitions, fears, and fantasies continuously. These simulations influence emotional expectation and behavioral readiness. Importantly, imagined experiences activate many of the same neural systems involved in actual perception and emotion. The body responds physiologically to internally simulated threat or desire because predictive systems treat vivid imagination as behaviorally relevant information. This overlap explains why alternate realities feel emotionally real despite conscious awareness of their fictional status. Memory contributes significantly to these constructions as well. Human memory is reconstructive rather than archival. Each act of remembering partially rebuilds experience using current emotional states, expectations, and narrative frameworks. Consequently, individuals do not merely recall the past; they continuously reinterpret it. Traumatic memory illustrates this process dramatically. Traumatic experiences often remain psychologically unresolved because overwhelming emotional activation disrupts normal integration. Instead of becoming stable autobiographical memory, fragments of sensation, fear, and bodily response continue intruding into present consciousness. The traumatized mind therefore creates alternate experiential realities in which past danger remains psychologically active within the present. Hypervigilance, flashbacks, and catastrophic anticipation all reflect predictive systems trapped within outdated survival models. From a biological perspective, this process is adaptive initially. The nervous system assumes that maintaining readiness for repeated threat increases survival probability. The problem emerges when the predicted danger no longer corresponds accurately to present conditions. Fantasy functions differently yet arises from related mechanisms. Fantasies allow temporary escape from emotional limitation, helplessness, shame, boredom, or dissatisfaction. By constructing alternate identities, relationships, or futures, the mind regulates emotional states difficult to tolerate directly. Importantly, fantasy is not inherently pathological. Imagination supports creativity, resilience, motivation, and symbolic exploration. Children especially rely heavily upon imaginative worlds during cognitive and emotional development. Pretend realities provide safe environments for experimenting with identity, power, fear, and social roles. However, under chronic stress or emotional deprivation, fantasy may become compensatory rather than exploratory. Individuals increasingly retreat into internally controlled realities because external life feels psychologically insufficient, unpredictable, or painful. The alternate reality begins regulating needs unmet by ordinary experience. Loneliness intensifies this tendency profoundly. Human consciousness evolved relationally. Emotional regulation depends heavily upon social connection, validation, and interpersonal synchronization. In the absence of stable relational environments, internally generated realities may partially replace external attachment structures. Imagined conversations, parasocial relationships, fictional identifications, and immersive fantasy worlds can therefore function psychologically as substitutes for unavailable emotional connection. These experiences may reduce distress temporarily while simultaneously increasing withdrawal from external relationships. Dissociation represents another important pathway into alternate reality construction. Dissociation occurs when integration among perception, memory, embodiment, and awareness becomes disrupted, often under overwhelming stress or trauma. Under such conditions, consciousness fragments into partially disconnected states. Depersonalization and derealization illustrate this fragmentation clearly. Individuals experiencing depersonalization feel detached from themselves, while derealization produces sensations that the external world is unreal, artificial, or dreamlike. These altered realities emerge because stress destabilizes perceptual integration systems responsible for maintaining coherent orientation. Paradoxically, dissociation often functions protectively. Emotional overwhelm becomes psychologically intolerable, so consciousness distances itself from direct experience. The resulting unreality reduces emotional intensity temporarily even while producing existential distress. Psychosis reflects more severe disruption of reality integration. Delusions and hallucinations may emerge when internally generated predictions become increasingly dominant over external sensory correction. Importantly, psychotic alternate realities are not random chaos. They are often highly meaningful attempts by the mind to organize overwhelming emotional and perceptual experiences into coherent narratives. Persecutory delusions, for example, frequently emerge within nervous systems organized around chronic fear, mistrust, or hypervigilance. The alternate reality reflects emotional truth expressed through distorted interpretation. The individual genuinely experiences threat even when the explanatory framework diverges from external consensus. This principle reveals something psychologically essential: alternate realities usually serve emotional coherence before factual accuracy. The mind prioritizes meaning, predictability, and survival over objective truth because these functions historically carried greater adaptive value. Internally coherent narratives reduce uncertainty even when inaccurate empirically. Dreams represent one of the most universal alternate realities humans experience. During dreaming, predictive and emotional systems generate immersive worlds largely independent of external sensory input. These dream realities often reorganize unresolved emotional material symbolically, blending memory fragments, fears, desires, and future anticipation. Dreaming demonstrates that consciousness naturally produces alternate experiential worlds even under ordinary biological conditions. The waking

Can Dreams Reshape Conscious Reality?
Dreams have occupied a psychologically mysterious position throughout human history. Unlike ordinary imagination, dreams possess a unique experiential intensity that often blurs the distinction between internal simulation and lived reality. Within dreams, individuals experience emotion, fear, embodiment, memory, desire, and narrative immersion with extraordinary immediacy. Even after awakening, certain dreams continue exerting emotional influence for hours, days, or even years. Some dreams alter relationships, shape beliefs, intensify anxieties, inspire creativity, or generate lasting existential reflection. This persistence raises an important psychological and neurocognitive question: can dreams reshape conscious reality, and if so, through what mechanisms do internally generated nocturnal experiences continue influencing waking perception long after sleep ends? To understand this process, it is first necessary to recognize that dreams are not psychologically separate from waking consciousness. Although dreaming and wakefulness involve different neurophysiological states, they emerge from the same cognitive architecture. Emotional memory, predictive processing, autobiographical reconstruction, symbolic association, and sensory simulation continue operating during sleep in altered configurations. Dreams therefore do not originate outside ordinary cognition; rather, they reveal cognition functioning under conditions where external sensory constraints are temporarily reduced. During wakefulness, perception is continuously anchored by external sensory input and environmental feedback. In dreams, however, internally generated imagery and emotion become the dominant source of experiential reality. The mind constructs complete environments, narratives, social interactions, and bodily experiences without direct external reference. Importantly, these constructions often feel entirely real while they occur. This realism reveals something fundamental about consciousness itself: the brain does not distinguish sharply between externally generated and internally generated realities at the level of immediate experience. Both waking perception and dreaming depend upon predictive simulation systems organizing sensation into coherent worlds. Dreams therefore demonstrate that reality perception is inherently constructive rather than purely receptive. One reason dreams influence waking life so powerfully involves emotional processing. Emotional intensity during dreams frequently exceeds ordinary waking emotional regulation because executive monitoring systems become partially reduced during REM sleep. Fear, longing, shame, grief, desire, and attachment therefore emerge with unusual directness and symbolic amplification. As a result, dreams often reactivate unresolved emotional conflicts more vividly than daytime cognition permits. Individuals may experience grief they suppress consciously, fears they rationalize away, or desires they avoid acknowledging while awake. The emotional authenticity of these experiences allows dreams to reshape waking self-perception by exposing hidden affective structures. Importantly, the brain encodes emotionally intense experiences preferentially regardless of whether they originate externally or internally. A terrifying dream may therefore leave physiological and mnemonic traces similar to those produced by actual threatening events. Heart rate changes, stress hormone activation, and emotional memory consolidation all contribute to the lingering realism of certain dreams. This process explains why nightmares can influence waking behavior long after awakening. The nervous system responds not merely to objective events but to emotionally convincing simulation. If a dream activates fear systems intensely enough, the resulting emotional memory may persist independently of conscious recognition that the event was fictional. Trauma research provides particularly important insight here. Traumatically stressed individuals frequently experience recurrent dreams involving danger, helplessness, or pursuit. These dreams do not merely replay memory literally; they reorganize emotional meaning repeatedly during sleep. In some cases the dreaming mind attempts integrating overwhelming experiences symbolically when direct conscious processing remains incomplete. Because emotional memory remains highly active during dreaming, traumatic dreams can reinforce hypervigilance and anxiety within waking life. The dream experience itself becomes incorporated into ongoing predictive models regarding danger and safety. Conscious reality is therefore reshaped indirectly through altered emotional expectation. Attachment systems are equally important in understanding dream influence. Human beings maintain complex internal representations of significant others, including memories, expectations, emotional associations, and relational patterns. During dreaming, these internal attachment models become highly active. As a result, dreams involving loved ones often feel psychologically significant because they reactivate emotional bonds with extraordinary immediacy. Bereaved individuals may dream vividly of deceased family members and awaken feeling as though genuine contact occurred. While neuroscience interprets such experiences through memory and attachment activation rather than supernatural visitation, the emotional effect can still profoundly alter waking consciousness. Dreams may provide temporary restoration of emotional continuity where physical absence exists. This explains why some individuals describe grief-related dreams as more psychologically transformative than conscious mourning itself. The dream permits experiential encounter rather than abstract reflection. Memory consolidation processes further strengthen dream influence. Sleep plays a crucial role in reorganizing emotional and autobiographical memory networks. During dreaming, fragments of past experiences, current concerns, and anticipated futures become recombined into novel symbolic structures. This recombination contributes to creativity, problem-solving, and emotional integration. However, it also means dreams can subtly modify waking interpretations of reality by reorganizing associative networks. A single emotionally powerful dream may alter how individuals perceive relationships, fears, ambitions, or identity because the dream changes emotional connections among memories and expectations. The symbolic dimension of dreaming is psychologically essential as well. Dreams rarely communicate through literal logic alone. Instead, they condense emotional themes into metaphorical imagery. Locations, figures, and events frequently represent broader psychological states rather than direct external realities. For example, recurring dreams of collapsing buildings may symbolize instability, vulnerability, or identity fragmentation rather than literal architectural fear. Yet because symbolic imagery bypasses ordinary rational filtering, the emotional impact may feel unusually profound. The dream appears to “know” something emotionally before conscious language fully articulates it. This sensation often leads individuals to attribute prophetic or mystical significance to dreams. In reality, dreams may appear predictive because they integrate subtle emotional information already present unconsciously. The dreaming mind continuously processes fears, desires, relational tensions, and environmental cues beneath awareness. Occasionally these implicit predictions later align with waking events, creating the impression of supernatural foresight. Pattern recognition biases intensify such interpretations. Humans remember emotionally meaningful coincidences far more vividly than failed predictions. Dreams coinciding with later events acquire enormous salience, while countless irrelevant dreams fade quickly from memory. Over time this selective recall creates exaggerated impressions regarding prophetic dreaming. Nevertheless, dreams genuinely influence future perception through expectation effects. A dream involving betrayal, catastrophe,

The Woman Who Never Felt Alone
In October 1978, a 29-year-old schoolteacher named Miriam Vale arrived in the remote coastal town of Whitby after accepting a temporary teaching position at a boarding academy located several kilometers outside the town center. According to employment records, Miriam was described as academically gifted, socially reserved, and psychologically stable. She had no documented psychiatric history, no criminal record, and no previous reports of unusual behavior. Within six months, however, local physicians, clergy, and eventually psychiatric specialists became involved in what residents later described as “the house incident,” a case that remained controversial not because of paranormal evidence, but because of the profound psychological transformation that unfolded within an apparently ordinary environment. The building Miriam rented stood near the edge of a cliff overlooking the North Sea. Constructed in the late nineteenth century, the house had remained mostly vacant for years except for occasional seasonal tenants. Residents described it as structurally sound but emotionally unsettling. Several previous occupants had reportedly left unexpectedly, though no officially documented events explained the pattern. When Miriam first moved into the house, her letters to friends contained no mention of fear or unusual experiences. In fact, she seemed fascinated by the isolation. One letter written two weeks after arrival stated: “It is quieter here than anywhere I have ever lived. At night you can hear only the wind and the sea. It feels detached from ordinary time.” This phrase—“detached from ordinary time”—would later appear repeatedly in her journals. During the first month, Miriam’s behavior reportedly remained normal. She taught classes regularly, socialized minimally but politely, and spent evenings reading or grading assignments at home. Yet subtle changes soon emerged. Coworkers noticed increasing fatigue. Miriam complained of fragmented sleep and persistent sensations that someone had entered the room moments before she turned around. Initially she dismissed these experiences humorously, attributing them to isolation and the unfamiliar acoustics of the old house. However, the sensations intensified. By December she reported hearing faint movements at night: footsteps in hallways, quiet knocking sounds, and occasional creaks that seemed rhythmically deliberate rather than random. Importantly, these sounds were not objectively verified. Neighbors heard nothing unusual. Yet to Miriam the noises felt increasingly organized, as though connected to intention. The psychological significance of this transition is crucial. Human perception is not passive recording but active interpretation. Under conditions of uncertainty, isolation, and heightened vigilance, ambiguous sensory stimuli often become integrated into meaningful narratives. The nervous system evolved specifically to detect agency within uncertain environments because missing genuine threats historically carried survival costs. Miriam did not initially interpret the experiences supernaturally. Her journals reveal ongoing attempts at rational explanation. She inspected pipes, windows, floorboards, and heating systems repeatedly. Yet each failed explanation increased rather than reduced her anxiety because uncertainty itself became psychologically destabilizing. One journal entry from January 4, 1979 read: “The worst part is not the sounds. It is the certainty that something almost becomes visible before disappearing again.” This statement reflects a phenomenon commonly associated with prolonged hypervigilance. Under chronic stress and perceptual ambiguity, attentional systems become hypersensitive to partial stimuli. Shadows, movement, peripheral distortions, and subtle environmental changes acquire exaggerated salience because the brain continuously searches for hidden threat. At the same time, isolation intensified Miriam’s introspective focus. Outside teaching hours she interacted with almost no one. Evenings were spent entirely alone inside an environment she increasingly associated with unease. Social isolation is psychologically important because interpersonal interaction normally stabilizes perception through shared reality-testing. Alone, internally generated interpretations gain increasing authority. By February Miriam reported a more disturbing development: she no longer merely sensed movement within the house but felt persistently accompanied. She described this sensation carefully. It was not visual hallucination in the conventional sense. She did not claim to see a figure standing clearly before her. Instead, she experienced what she called “proximity without image”—the absolute conviction that another presence occupied nearby space. The sensation appeared strongest in transitional areas: hallways, staircases, doorways, and the room beside her bedroom, which she eventually stopped entering altogether. Modern neuroscience offers important insight into such experiences. The human brain continuously integrates sensory, proprioceptive, and spatial information into a coherent sense of self-location. Under conditions involving stress, sleep disruption, isolation, or perceptual instability, these integration systems may become disturbed. Internal bodily awareness can become partially externalized, producing the sensation that another being exists nearby. Research involving neurological stimulation has even artificially induced “presence hallucinations” in laboratory settings, where participants suddenly feel an invisible person standing close behind them despite knowing nobody is present. For Miriam, however, the experience felt entirely real. Her sleep deteriorated severely. She began waking repeatedly around 3:00 a.m., convinced someone had just spoken softly near her bed. Yet no clear words were ever identifiable. The sounds existed at the threshold between perception and interpretation. This ambiguity became psychologically devastating because uncertainty prevented cognitive closure. Clear hallucinations can sometimes be recognized as pathological. Ambiguous experiences remain more destabilizing because they resist definitive categorization. Miriam could neither confirm nor fully dismiss what she felt. Coworkers later described visible changes in her appearance. She lost weight rapidly, appeared emotionally flattened during conversations, and startled easily at minor noises. Yet she remained intellectually coherent. This coherence made her experiences more disturbing to listeners because she did not resemble stereotypical depictions of psychosis. One colleague later stated: “She spoke about it calmly. That was what frightened people. She sounded like someone describing weather, not madness.” As weeks passed, Miriam developed increasingly elaborate interpretations regarding the house itself. She became convinced the building retained emotional traces from previous occupants. She described certain rooms as “holding memory” in ways difficult to articulate precisely. Importantly, these beliefs emerged gradually from emotional experience rather than abstract paranormal fascination. The house had become psychologically charged through repeated association with fear, uncertainty, insomnia, and hypervigilance. Over time, the environment itself triggered anticipatory arousal automatically. This process illustrates associative conditioning at work. Places acquire emotional meaning through repeated pairings with particular physiological states. Eventually the environment alone becomes
The Man Who Heard Thoughts
In the winter of 1957, a 34-year-old radio technician named Adrian Keller was admitted to a psychiatric clinic on the outskirts of Zurich after several months of increasingly disturbing experiences that he insisted were not hallucinations, but evidence of direct mental transmission between people. According to medical notes recorded during his first interviews, Adrian did not initially present with overt psychosis in the dramatic sense often portrayed in popular culture. He was coherent, articulate, and capable of discussing technical subjects with precision. Staff described him as unusually observant and emotionally restrained. What concerned clinicians was not disorganized behavior, but the intensity with which he described an expanding conviction: he believed he had begun hearing fragments of other people’s thoughts. The experiences reportedly began gradually. At first, Adrian noticed what he interpreted as improbable coincidences during conversations at work. He would internally formulate a sentence moments before a colleague spoke nearly identical words aloud. Sometimes he anticipated jokes, comments, or emotional reactions with unsettling accuracy. Initially he dismissed these incidents as intuition. Yet over time the frequency of such moments appeared, at least subjectively, to increase. He began monitoring them carefully. In notebooks later recovered from his apartment, Adrian documented hundreds of interactions in meticulous detail. He recorded timestamps, locations, exact phrases, environmental conditions, and emotional states preceding each event. Many entries reflected ordinary conversational prediction rather than anything supernatural. However, Adrian interpreted the accumulation itself as statistically impossible. One passage written in March 1957 stated: “It no longer feels accidental. The thoughts arrive before the voices. Sometimes not as words exactly, but as pressure, direction, emotional shape. Then the person speaks, and the external sentence matches what already formed internally.” His coworkers initially perceived these observations as eccentric but harmless. Adrian had always been introspective and intensely analytical. Yet subtle behavioral changes soon emerged. He became socially withdrawn and increasingly hypervigilant during interactions. He stared at others for prolonged periods, as though attempting to detect invisible signals beneath ordinary communication. At work he complained about “mental interference” in crowded rooms. Cafeterias, train stations, and public gatherings reportedly became overwhelming because he felt exposed to fragments of surrounding consciousness. He described the experience not as hearing literal voices through the ears, but as receiving abrupt impressions that appeared alien to his ordinary stream of thought. Importantly, Adrian retained partial insight during early stages. He repeatedly acknowledged uncertainty regarding the experiences. In several diary entries he questioned whether exhaustion or stress might be distorting his perception. Yet these moments of doubt gradually weakened as emotional conviction intensified. The transition from curiosity to certainty appeared closely linked to a specific event occurring in late April. One evening Adrian attended a small gathering hosted by a colleague. During a conversation, he reportedly experienced what he later described as “complete overlap” with another individual’s mind. He claimed that while standing across the room from a woman named Elise, he suddenly became overwhelmed by a vivid emotional impression consisting of grief, anxiety, and imagery involving a hospital corridor. Seconds later, according to Adrian, Elise abruptly mentioned her mother’s recent hospitalization. Witnesses later confirmed that Elise had indeed spoken about family illness during the conversation. However, there was no evidence that Adrian possessed information unavailable through ordinary contextual cues. Yet for Adrian, the timing created overwhelming emotional confirmation. Afterward he wrote: “That was the moment certainty arrived. Before, there was probability. After tonight, probability no longer explains it.” Following this event, Adrian’s interpretations became increasingly elaborate. He concluded that most humans unconsciously transmitted emotional and cognitive signals continuously, but that social conditioning prevented awareness of the process. He believed stress, electromagnetic exposure, and emotional sensitivity had somehow altered his perceptual threshold, allowing him to perceive what others ignored. The psychological structure of his belief is clinically significant because it did not emerge randomly. It evolved gradually through interactions among attention, pattern detection, emotional salience, and interpretive reinforcement. Modern cognitive psychology offers important insight into how such convictions can develop without deliberate fabrication. Human beings possess highly advanced predictive social cognition systems. Through subtle facial cues, body language, speech timing, and contextual inference, individuals constantly anticipate one another’s reactions unconsciously. Under ordinary conditions these predictions remain invisible because the underlying perceptual mechanisms never reach awareness. However, certain conditions can destabilize the boundary between intuition and perceived external reception. Adrian’s journals strongly suggest progressive hyper-attunement to social cues. He became intensely focused on interpersonal micro-patterns that most people process automatically. This hyperfocus likely amplified his predictive accuracy in some interactions. Yet because the cognitive mechanisms remained unconscious, the successful predictions felt externally sourced rather than internally inferred. At the same time, selective attention and confirmation bias reinforced the developing system. Adrian recorded successful anticipations obsessively while largely ignoring failed predictions. Over time this produced a self-validating narrative in which evidence appeared overwhelmingly supportive. Clinicians later noted additional contributing factors. During psychiatric evaluation, Adrian disclosed severe insomnia lasting nearly four months before hospitalization. He slept irregularly, often remaining awake until dawn documenting observations and replaying conversations mentally. Sleep deprivation profoundly alters cognitive integration. Research now demonstrates that prolonged sleep disruption increases emotional reactivity, perceptual instability, dissociative symptoms, and aberrant salience detection. Under such conditions, ordinary experiences can acquire exaggerated significance. Coincidences feel revelatory. Intuitive impressions feel externally imposed. Emotional certainty intensifies independently of objective evidence. Adrian also reported longstanding social isolation beginning years earlier after the death of his younger brother in a climbing accident near Swiss Alps. Family interviews suggested he never processed the loss fully. Instead, he withdrew emotionally while becoming increasingly absorbed in technical and philosophical subjects involving communication systems and electromagnetic theory. This detail became psychologically important because grief often reorganizes attachment and perceptual systems in subtle ways. Bereaved individuals frequently report heightened sensitivity to symbolic coincidence, emotional resonance, and experiences interpreted as invisible connection. The mind continues searching for relational continuity even after physical absence. In Adrian’s case, unresolved grief may have intensified both emotional sensitivity and the longing for forms of communication transcending