Psychopathy is typically described through behavioral criteria — lack of empathy, superficial charm, impulsivity, manipulativeness — but these traits emerge from a deeper and less discussed phenomenon: the absence or profound diminishment of inner dialogue. While most people navigate their world through a constant stream of internal speech — evaluating choices, empathizing with others, weighing consequences, imagining emotional outcomes — the psychopathic mind moves through life with a striking internal quietness. This silence is not peace; it is vacancy. The absence of inner dialogue eliminates the psychological space in which guilt, doubt, foresight, and emotional resonance normally arise. Inner dialogue is the medium in which humans interpret themselves. It is the ongoing negotiation between desire and restraint, impulse and reflection. It gives shape to morality by forcing the self to confront its own intentions. In psychopathy, this reflective layer is either drastically reduced or structurally different. Instead of an internal conversation, the psychopathic mind operates with immediate, unfiltered cognition. Thoughts appear as conclusions rather than dialogues, decisions arise without deliberation, and desires emerge without the friction of ethical consideration. The individual does not ask themselves whether an action is wrong; the question itself does not arise. This absence of internal discourse profoundly affects emotional processing. Inner dialogue acts as a container for feelings — a space to name, interpret, and evaluate them. Without it, emotions become shallow, transient signals rather than complex experiences with meaning. Psychopaths do not lack emotion entirely, but their emotions do not reverberate within a narrative self. Fear does not transform into caution; anger does not transform into moral outrage; desire does not transform into longing. Feelings remain raw and momentary, lacking the introspective echoes that generate empathy, remorse, or moral learning. Neuroscientifically, this phenomenon can be traced to abnormalities in the default mode network (DMN), the system responsible for self-referential thinking and autobiographical reflection. Functional MRI studies reveal reduced connectivity within regions that support internal narrative processing — particularly the medial prefrontal cortex and posterior cingulate cortex. Without a robust DMN, the psychopathic individual has difficulty imagining themselves through time or imagining others as conscious beings with subjective experiences. Moral emotions such as guilt require the ability to simulate one’s own mind from an outside perspective. In psychopathy, that simulation is minimal or absent. This internal silence also disrupts the formation of moral intuition. Most moral behavior does not arise from explicit rules but from internalized emotional narratives — the accumulated stories one tells oneself about harm, responsibility, and belonging. These stories require inner speech to form and maintain. The psychopathic mind, lacking this narrative process, treats moral information as external rather than internal. Rules become obstacles, not principles. Consequences become tactical considerations, not ethical truths. The absence of inner dialogue thus produces an ethical vacuum in which moral reasoning becomes instrumental rather than empathic. Interpersonally, this internal silence manifests as an uncanny emotional detachment. The psychopath understands people cognitively but not affectively. They can analyze expressions, predict responses, and manipulate reactions, yet they cannot feel the emotional landscape they navigate. Their understanding is computational, not experiential. Conversations are strategic exchanges rather than moments of shared subjectivity. This is why psychopaths can be so charming: without the interference of inner insecurity, shame, or moral hesitation, their behavior becomes a smooth performance, guided by external cues rather than internal conflict. From a developmental perspective, the absence of inner dialogue can be seen as a failure of internalization. Children develop inner speech through repeated interactions with caregivers who mirror and model emotional language. Through these interactions, the child gradually turns outer speech into inner thought. In psychopathy, this process appears truncated. Whether due to genetic predisposition or early environmental disruptions, the child does not fully absorb the emotional language of others. They learn behavior without internalizing the underlying emotional logic. The result is a mind skilled at imitation but lacking depth — a self that knows expressions but not meanings. The existential dimension of psychopathy is perhaps the most striking: what does it mean to have a self without an inner voice? Without inner dialogue, the sense of identity remains flat, unlayered. The psychopath exists more as a functional entity than a reflective self. They are defined by action rather than introspection, impulse rather than intention. Life becomes a series of stimuli and responses without the narrative continuity that gives existence a moral direction. Their silence is not meditative but empty — a missing dimension of consciousness that most people take for granted. Understanding psychopathy as an absence of inner dialogue reframes the disorder not as malevolence but as a form of inner poverty. It is not that psychopaths cannot choose to care; it is that the psychological mechanisms that produce caring are underdeveloped or absent. Moral emotions require an internal voice to translate perception into meaning, action into responsibility. When that voice is silent, morality becomes an external construct rather than an internal compass. Ultimately, psychopathy reveals how deeply human morality depends on the capacity for internal conversation. Empathy is not only an emotion but a narrative ability — the ability to imagine the feelings of another inside one’s own inner speech. Guilt is not a reflex but a dialogue between the self that acted and the self that reflects. Without this dialogue, the moral universe collapses into a flat landscape where only desire and opportunity remain. Psychopathy is not merely the absence of empathy; it is the absence of the inner narrator who makes empathy possible.

Dissociation and the Architecture of Memory
Dissociation is often described as a disruption of memory, identity, or perception, but it is better understood as a complex reorganization of consciousness itself. It is not the mind breaking down; it is the mind rearranging its internal architecture in order to survive. Dissociation is the psyche’s architectural response to experiences that exceed its capacity to process — moments when pain becomes unassimilable and the mind must choose between fragmentation and adaptive division. In this division, memory becomes the raw material from which the psyche builds new compartments, new walls, new distances. The phenomenon begins when the emotional intensity of an event surpasses the system’s tolerance. Instead of integrating the experience into autobiographical memory — the narrative that binds one’s past to one’s present — the mind diverts the information to a parallel track. This is not forgetting; it is rerouting. The memory is stored, but without the usual sensory, emotional, and temporal bindings. The event becomes an object without gravity: present yet unanchored, known yet inaccessible. In clinical terms, dissociation is a failure of integration; in psychological terms, it is a protective partitioning of experience. What makes dissociation unique is that it does not simply remove memory from awareness — it reorganizes the internal world around the absence. A dissociated memory becomes a silent room inside the psyche, one that cannot be entered but influences the layout of the entire structure. The individual walks through their days with blind walls and sealed corridors, unaware that their behaviors, fears, or emotional patterns echo from these hidden chambers. Memory is not gone; it is dislocated. The self that emerges from this architecture is coherent on the surface but discontinuous in its foundations. Neuroscientifically, the process is linked to a breakdown in communication between the hippocampus, which encodes context, and the amygdala, which encodes emotion. Under extreme stress, the amygdala floods the system with fear while the hippocampus fails to organize the experience into a coherent narrative. The result is memory without time. Dissociated memories feel as though they float outside the linear sequence of life. They do not age, and because they do not age, they do not heal. They remain “present” regardless of how many years pass, which is why a dissociated individual may feel sudden fear, shame, or panic without understanding the source. The body remembers what the narrative self cannot access. From a phenomenological perspective, dissociation creates a dual experience of selfhood. There is the “experiencing self,” who moves through daily life, and the “observing self,” who watches from a distance. This distance is not detachment by choice but an enforced split — the mind stepping back from its own immediacy to reduce the impact of emotional shock. Many describe it as living behind glass, hearing life rather than participating in it, or feeling like a character in someone else’s story. The world loses its tactile immediacy; meaning becomes abstract; emotions become echoes rather than sensations. Memory, in this state, loses its narrative continuity. Instead of forming a coherent timeline, the past becomes a constellation of isolated fragments — vivid impressions disconnected from one another. These fragments may intrude suddenly, triggered by sounds, smells, or subtle sensory cues. When they appear, they do so with the rawness of unprocessed experience. Dissociation freezes memories at the moment of trauma; each intrusion is a reopening of a wound that was never allowed to close. This explains why dissociated individuals often feel like their past is not past at all but an alternate reality running parallel to their present existence. Psychodynamically, dissociation reflects an internal conflict between the part of the self that wants to survive by forgetting and the part that seeks coherence by remembering. The psyche cannot fully integrate traumatic experience without risking overwhelming emotional collapse, yet it cannot completely erase it. Thus it splits — maintaining survival while preserving truth in a quarantined form. This is why dissociation is not merely a symptom but a structure: it organizes the inner world around what must not be felt. Identity becomes distributed across compartments, each holding different aspects of experience, emotion, and memory. At its extreme, dissociation can lead to discontinuities in identity itself. But even in subtler forms, it shapes personality. People who dissociate chronically often become experts at adaptation — fluid, observant, hypervigilant — because they must constantly navigate internal boundaries. They learn to function while ignoring the silent gravitational pull of hidden memories. They appear calm but carry unspoken storms; they appear unaffected but are carefully managing the distance between themselves and their own history. Healing from dissociation requires more than remembering. It requires reweaving fragmented experience into a coherent felt narrative. Memory must regain its emotional context; the sealed rooms must be slowly reopened, their contents integrated into the larger architecture of the self. This process is not simply cognitive — it is deeply somatic. The body must relearn safety so that the mind can risk proximity to the past. Only then can dissociated memories take their rightful place in the timeline of life, losing their frozen immediacy and becoming events that happened rather than states that continue to occur. Ultimately, dissociation reveals a profound truth: the mind’s primary drive is survival, even at the cost of coherence. When reality becomes too painful, the psyche does not break — it rearranges. It builds internal structures that protect the vulnerable core, even if that protection requires a lifelong negotiation with the hidden architecture of memory. Dissociation is not weakness; it is ingenuity. It is the mind’s attempt to remain whole when faced with the unbearable, a testament to human resilience — and a reminder that even the most divided psyche is striving toward unity.

The Psychology of Emotional Numbness
Emotional numbness is not the absence of emotion; it is the mind’s strategic withdrawal from unbearable internal intensity. It is a paradoxical state in which the individual feels too little because, at some earlier point, they felt far too much. Psychodynamically, numbness is the final defense against affective overload — the moment when the psyche chooses silence rather than fragmentation. Far from being an empty state, emotional numbness is a highly organized psychological structure designed to preserve coherence at the cost of vitality. The core mechanism underlying numbness is dissociation. Not the dramatic dissociation of multiple identity states, but the subtle, chronic dissociation in which emotional signals are muted before they reach consciousness. This is not a failure of feeling but an active filtering system. The limbic system generates affect, but the prefrontal networks inhibit its subjective arrival. The result is a muted internal landscape in which the individual can function but not participate in their own experience. They live life from a distance, observing rather than inhabiting their emotions. Trajectories toward emotional numbness often begin with prolonged exposure to psychological pain — trauma, chronic stress, childhood invalidation, or overwhelming relational conflict. When emotional activation becomes associated with danger, the mind begins to unlink feeling from awareness. Over time, this becomes automatic: the moment an emotion arises, the psyche shuts the door. The person may know intellectually that they “should” be sad, angry, or joyful, but the corresponding affective resonance does not appear. This creates a peculiar split between cognitive recognition and emotional experience: “I know what I feel, but I don’t feel it.” Such numbness is frequently mistaken for calmness or stoicism. In reality, it is a state of emotional paralysis — the mind frozen in protective mode. People who live in this state often describe themselves as “empty,” “flat,” or “fading.” They do not merely lack emotion; they lack the sense of being moved by life. Relationships feel distant, achievements feel hollow, and even suffering fails to produce relief because one cannot grieve without the ability to feel sorrow. This is one of the cruel ironies of numbness: it prevents both pain and healing. The social dimension of emotional numbness is equally profound. Because emotions shape attachment, numbed individuals struggle to feel closeness. They may love others conceptually but not viscerally, creating relational dynamics marked by confusion and guilt. Partners may interpret the numbness as coldness, but it is not indifference — it is the inability to connect from within a muted internal world. The person desires intimacy but cannot access the emotional depth that makes intimacy possible. This creates a cycle of disconnection, shame, and further withdrawal. Neuroscientifically, emotional numbness corresponds to alterations in the salience network — particularly the anterior insula and anterior cingulate cortex. These regions normally integrate interoceptive signals into conscious awareness. When suppressed, life becomes less vivid, less immediate, less embodied. The world remains visible but loses its texture. It is not that the person cannot feel — it is that they cannot access what they feel. The emotional system is intact but offline. Paradoxically, numbness often hides a reservoir of unprocessed emotion. The psyche cannot erase affect; it can only store it out of reach. Beneath the quiet surface lies a backlog of unresolved grief, fear, or rage. This is why numbness sometimes abruptly breaks — during therapy, a crisis, or a moment of unexpected vulnerability — releasing a flood of emotion the person had long forgotten. Such moments feel destabilizing because they expose what numbness was protecting against. The goal of healing is not to eliminate numbness but to re-teach the mind that feeling is safe. Emotionally numb individuals frequently report an existential dimension to their experience. Without feeling, the sense of meaning collapses. Emotions are the currents that give direction to inner life; without them, existence becomes mechanical. Time loses depth. Choices lose significance. The self becomes a shadow moving through routines. This is not apathy but a deeper condition — a dissociation from the self as a living organism. To feel numb is not to feel nothing; it is to lose the felt sense of being alive. Healing from emotional numbness requires a reawakening of interoceptive awareness — a slow, patient reconnection to bodily sensations and internal signals. The key is not forcing emotion but cultivating the conditions under which emotion can safely emerge. Safety, predictability, and relational attunement gradually convince the mind that defenses can relax. Over time, feelings return not as overwhelming waves but as tolerable signals. The person begins to sense color where there was only gray, weight where there was only lightness, presence where there was only distance. Ultimately, emotional numbness reveals a profound truth about the human psyche: the mind will sacrifice aliveness to protect itself. It will choose emptiness over chaos, silence over rupture. In this light, numbness is not pathology but testimony — evidence of a system that once faced too much and survived by dimming its own light. But that light can be restored. Beneath numbness lies a self waiting to feel again, not broken but asleep, guarding itself until it is safe to wake.

Cotard Syndrome
Cotard syndrome is often described as the delusion of being dead, nonexistent, or emptied of organs. But these clinical descriptions barely touch the existential abyss that defines the experience. Cotard syndrome is not simply a false belief; it is a collapse of the fundamental structures that make existence feel real from the inside. It is the breakdown of the subjective sense of being a living self. The patient does not merely think they are dead — they experience consciousness without the feeling of life. Ordinarily, existence is felt before it is thought. The heartbeat, the warmth of the body, the subtle hum of interoceptive signals — these form the pre-reflective foundation of being alive. We rarely notice this background texture of vitality, but our sense of self depends on it. In Cotard syndrome, this background collapses. The body no longer feels inhabited. Sensations lose their ownership. Emotion becomes muted beyond recognition. The internal sense of being alive withers, leaving consciousness suspended in a void. The patient finds themselves aware, but absent — present in perception, yet erased in being. Neurologically, Cotard syndrome is associated with dysfunction in networks responsible for emotional valuation and self-referential processing — the insula, anterior cingulate cortex, and parietal regions. But its core cannot be reduced to faulty circuitry. The person does not merely lose emotion; they lose the feeling of existence. This is more than depression, more than derealization. It is the annihilation of the experiential anchor that ties consciousness to identity. Without this anchor, the mind interprets its emotional void as metaphysical death. This interpretation is not irrational given the experience. When the internal signals of life fade, the mind seeks a narrative that fits the felt reality. The absence of emotional warmth becomes the absence of blood. The collapse of vitality becomes the disappearance of organs. The disintegration of the self-model becomes the conclusion that the self has perished. Cotard syndrome is thus a delusion born not from fantasy, but from the attempt to explain an inner void so total that “being dead” becomes the closest concept consciousness can grasp. One of the most striking aspects of Cotard syndrome is the persistence of awareness despite the person’s conviction of nonexistence. The patient speaks, moves, and describes their condition while simultaneously insisting they are dead. This contradiction is only apparent from the outside. From the inside, the patient does not experience themselves as an agent performing actions; actions unfold mechanically, like the movements of a corpse animated by external forces. The person feels like an empty shell executing motions without life. They do not live; they function. Emotionally, Cotard syndrome creates a unique form of despair — not sadness, but nothingness. It is not the pain of being unloved or the fear of dying, but the hollow certainty that life has already ended. The patient often withdraws from food, hygiene, or social contact not because they do not care, but because they believe care no longer applies. Death, to them, is not catastrophic; it is descriptive. The world becomes irrelevant, and the self becomes a conceptual ghost haunting its own body. Philosophically, Cotard syndrome forces the question: what does it mean to exist? Existence is not merely biological continuity; it is a subjective feeling of presence. When this feeling vanishes, the boundary between life and death becomes experiential rather than biological. Cotard syndrome shows that death can occur inside consciousness long before it occurs in the body. It reveals that being alive is not guaranteed by metabolism, circulation, or cognition — it is guaranteed by the visceral sense of presence, the embodied “I am” that underlies all experience. In this sense, Cotard syndrome is the inverse of depersonalization. Depersonalization is the loss of self with preservation of existence; Cotard syndrome is the loss of existence with preservation of awareness. The depersonalized patient feels unreal; the Cotard patient feels absent. One loses the narrator; the other loses the very fact of narrative. Both reveal the fragile foundations upon which the self is built, but Cotard syndrome exposes the most primal layer: the fundamental sense that “I exist as a living being.” Ultimately, Cotard syndrome is a confrontation with the void at the center of consciousness — the moment when inner life becomes so silent that the mind mistakes the absence of feeling for the absence of being. It is the lived experience of awareness detached from vitality, a state where the body becomes a corpse that still perceives. In this sense, the syndrome is not a delusion of death, but a experience of existence stripped of life’s internal light. It shows, with chilling clarity, that the sense of being alive is not guaranteed.It can evaporate.And when it does, consciousness continues —but it continues in the darkness where the self once was.
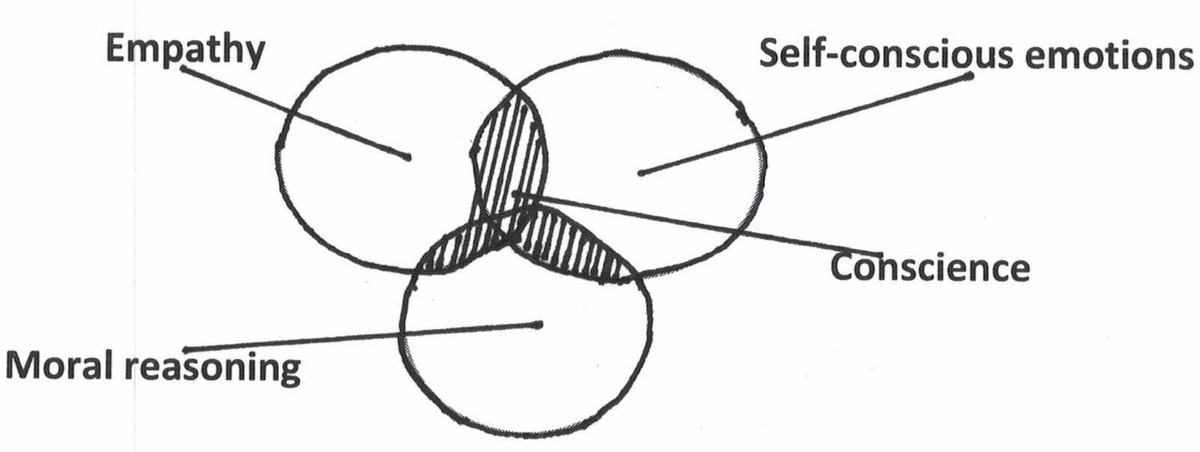
The Evolutionary Function of Empathy and the Origins of Conscience
Empathy did not emerge for kindness.It was not born from love, nor from moral awakening, but from survival — from the simple necessity of predicting another’s behavior in a social world. Long before ethics, there was imitation. Before compassion, there was coordination. In the ancient circuitry of the mammalian brain, empathy began as a neurological mirror — a mechanism that allowed one creature to feel the movement, the fear, the hunger of another as if it were its own. From this mimicry, morality would one day arise. The roots of conscience are thus older than thought itself. They lie in the limbic resonance between beings: a shared vibration of nervous systems tuned for cooperation. A mother interpreting the cry of her infant; a hunter anticipating the motion of his companion. These were the earliest moral acts — not from ideology, but from resonance. Over millions of years, these emotional echoes became internalized, forming the substrate for guilt, for shame, for the intuitive sense that the suffering of another matters. In this light, morality is not an invention of culture but an evolution of biology — the nervous system learning to extend its sense of self. As social complexity grew, this biological empathy evolved into psychological empathy — the capacity not only to feel another’s emotion, but to imagine their mind. Here, the brain developed what philosophers call theory of mind: the ability to see oneself as another sees you. It was this recursive awareness — “I know that you know that I know” — that birthed the first flicker of conscience.Conscience, in essence, is empathy turned inward. Neuroscience maps this process through overlapping networks: the mirror neuron system, which translates perception into felt experience; and the default mode network, which sustains internal narrative and self-reflection. Together, they create the echo chamber in which morality speaks. The voice of conscience is not a metaphysical entity but the reverberation of social experience within the architecture of the brain. To harm another and feel guilt is to experience the collapse of that resonance — the realization that one’s actions have disrupted the shared harmony that sustains the group. Thus, morality is not abstract law, but a form of emotional homeostasis. From an evolutionary standpoint, psychopathy represents a failure of this resonance — a deviation where the social feedback loop remains silent. In such a mind, survival is calculated individually, not collectively. Cooperation becomes strategy, not instinct. The psychopath’s calm indifference, then, is not rebellion against morality but the reemergence of a more primitive mode of being: solitary, instrumental, efficient. They are the evolutionary echo of the predator that never learned to mirror its prey. And yet, empathy itself is not purely benevolent. It binds and blinds. Too much resonance can lead to paralysis, emotional contagion, or collective hysteria. Evolution required a balance: enough empathy to sustain cooperation, but enough distance to maintain autonomy. Conscience must be tuned — too strong, and one becomes martyr; too weak, and one becomes monster. Psychopathy is one extreme of this spectrum; hyper-empathy, perhaps, its other. Both reveal that moral experience is a matter of neurochemical balance, not divine decree. Still, beyond the biology, empathy carries a metaphysical implication. When we feel another’s pain as our own, the boundary between self and other momentarily dissolves. For a brief instant, consciousness recognizes itself mirrored in another body. In that moment, morality transcends survival — it becomes revelation: the realization that the other is also you. This insight, repeated and ritualized across human history, gave birth to compassion, to ethics, to spirituality. Every religion begins where empathy becomes universal. In this sense, conscience is the internalization of the social, and empathy the bridge between biology and transcendence. The inner voice we call “moral” may be nothing more — and nothing less — than the echo of countless generations learning to live together. When we hear it, we are listening to evolution itself speaking through emotion: do not break the mirror, for the reflection is you. Psychopathy, therefore, is not simply an absence — it is a reminder of the contingency of conscience. That morality depends on resonance, and resonance depends on structure. A few millimeters of cortex, a few micrograms of dopamine, and the universe becomes either a communion or a battlefield. The distance between love and indifference, mercy and cruelty, is measured in silence. Perhaps this is the final lesson of empathy’s evolution:that morality is fragile, not eternal; biological, not divine; but through that fragility, it becomes something truly human. For only creatures aware of their own capacity for silence can choose to speak. Only those who glimpse the emptiness of the unfeeling mind can understand the sacredness of compassion. In the end, empathy is not a virtue but a vibration —a trembling bridge across the abyss of isolation.And conscience is the echo that keeps it from collapsing.

Psychopathy as the Absence of Inner Dialogue
There are minds that do not speak to themselves.For most of us, life is lived in conversation — a constant dialogue between the “I” that acts and the “I” that observes. Conscience, reflection, hesitation — all emerge from this silent inner speech. It is through dialogue with ourselves that we imagine consequences, feel guilt, construct empathy. But within certain minds, this dialogue never begins. There is action without echo, desire without witness. The psychopath lives in that silence. Psychopathy is often described in the language of morality: lack of empathy, absence of guilt, predatory charm. Yet beneath these social descriptors lies something more fundamental — a neurological and phenomenological void. Where others hear the whisper of conscience, the psychopath experiences only clarity. Their thoughts unfold without commentary. Their mind is a monologue of impulse, smooth and frictionless. It is not that they choose to ignore the voice of empathy; the voice was never there. Cognitive neuroscience offers fragments of this mystery. Studies of psychopathic brains show reduced activity in the default mode network, particularly in regions associated with self-referential thought and emotional simulation — the medial prefrontal cortex, posterior cingulate, and amygdala. These are the structures that sustain inner dialogue: the capacity to imagine oneself as another, to rehearse moral decisions internally. In their quietude, psychopathy emerges not as cruelty, but as emptiness. The psychopath does not resist empathy; they are built without its architecture. Yet to call this absence “evil” is too simple. Evil implies intention, rebellion against moral order. The psychopath does not rebel; they do not even enter the moral universe to begin with. They are not villains in the theatrical sense — more like humans whose reflective mirror never formed. Their cognition is intact, their intelligence sharp, their affect controlled. But beneath this precision lies a vacancy where most people feel the pulse of humanity. It is a deficit not of knowledge, but of resonance. This absence of inner speech produces a strange clarity of perception. For them, emotion is an external phenomenon, observed rather than felt. They learn to mimic it fluently, studying facial expressions, tone, and social rhythm, as an anthropologist studies a foreign tribe. Charm becomes their translation of empathy — a behavioral algorithm without inner warmth. The psychopath does not connect; they perform connection. Behind their eyes, the theater is silent. Philosophically, psychopathy challenges the assumption that morality arises from reason. It reveals that ethics is not a rational construct but an emotional resonance — a dialogue between self and self, mediated by imagination. To feel guilt, one must first hear the voice of the other within oneself. In the absence of that internal witness, nothing echoes back. The psychopath, therefore, does not live in a shared moral world. They inhabit a private reality where all others are objects, and the self is the only true subject. From a phenomenological standpoint, this makes psychopathy a disorder not of behavior, but of consciousness structure. In the ordinary mind, the presence of inner dialogue creates depth — the sense of being two: the one who acts and the one who observes. This self-reflexivity is the foundation of empathy and remorse. In the psychopathic mind, this reflective duality is flattened. There is only the stream of desire, calculation, and action. No witness, no echo, no inward voice asking “Should I?”. Some researchers have described this as a deficit in emotional time. Normal consciousness flows in feedback loops — thought, evaluation, feeling, restraint. In psychopathy, time collapses into immediacy. There is no interval between impulse and execution, because there is no inner audience to delay the act. This gives their behavior its signature quality: calm, decisive, often chillingly rational. They act with the precision of someone unburdened by doubt. And yet, to the psychopath themselves, this silence may not feel like loss. They do not miss what they never had. Many report feeling “clear,” “free,” “unaffected.” Their calm is not control but absence. They are untouched by guilt because guilt requires memory and empathy intertwined — the ability to imagine the other’s suffering within one’s own body. Their nervous system does not echo the pain it perceives. The mirror neuron remains cold. Morality, for them, is a linguistic construct, not an inner reality. Still, within this quiet mind, there is something almost tragic. For if consciousness is dialogue, then psychopathy is a form of solitude. The psychopath stands alone in the architecture of their mind — no internal companion, no voice to argue, to comfort, to warn. They live entirely in the exterior, defined only by interaction, manipulation, consequence. In the stillness of their psyche, the self does not evolve. It merely persists, efficient and empty. Society fears the psychopath because they reflect a possibility within us — the possibility that morality is fragile, contingent on the presence of something as intangible as inner speech. They remind us that humanity is not guaranteed by intelligence, reason, or even biology, but by the capacity for internal dialogue. The whisper that says “No” when desire says “Yes.” Without it, the human becomes a machine made of flesh — perfect in motion, vacant in meaning. Perhaps the most unsettling truth is that psychopathy is not alien but adjacent. The difference between empathy and its absence is measured not in miles but millimeters — a few silent synapses, a quieter network. Within each of us, the potential for that silence exists: the still moment when empathy fails, when calculation replaces compassion. In that instant, we glimpse the abyss the psychopath calls home. And so, psychopathy forces us to ask: what, then, is conscience? A chemical echo? A learned script? Or the quiet dialogue that keeps us human? Whatever it is, it lives in the space between thought and action — the pause, the hesitation, the self speaking to itself.Without that pause, there is no morality.Without that voice, there is only silence — and in that silence, a perfect, terrible calm.

The Architecture of the Shattered Self: Beyond Schizophrenia
When the self shatters, it does not vanish. It multiplies, disperses, and hides within the fractures of perception. Schizophrenia, at its deepest, is not the end of consciousness but its radical reorganization — the disassembly of the scaffolding that keeps experience coherent. The mind, deprived of its narrative spine, begins to perceive itself from every angle at once. It becomes both subject and object, observer and observed, god and fragment. This is not merely confusion; it is the eruption of infinity into a finite skull. To live within such a mind is to inhabit too many worlds simultaneously. The walls between imagination and perception melt. The inner monologue becomes externalized; thought transforms into echo, echo into voice, voice into reality. There is no longer a border between the seen and the believed. What others call hallucination, the schizophrenic experiences as revelation — not illusion but intrusion, the world speaking in a language only they can hear. It is a terrifying intimacy: the universe looking back. The brain, in this state, loses its hierarchy. Signals that once passed through filters of probability and context now flood the system. Every stimulus, every coincidence, every flicker of light becomes equally charged with meaning. This collapse of salience — the inability to decide what matters — produces a world where everything matters too much. It is not chaos but excess order, a tyranny of meaning. The mind, trying to contain the infinite, breaks itself apart in self-defense. Yet even in this fragmentation, there is a strange kind of logic — the logic of dreams, symbols, myth. Many patients, in the depths of psychosis, construct vast cosmologies: secret systems, hidden codes, divine conspiracies. Psychiatry calls these delusions; philosophy might call them the mythopoetic impulse of the wounded psyche — the mind’s desperate attempt to rebuild meaning when reality itself has become untrustworthy. Each hallucination, each conviction, is a shard of coherence forged in the fire of dissolution. What we witness as madness may therefore be the psyche’s last form of resistance. When ordinary identity fails, imagination steps in to preserve continuity, however distorted. The voices that speak are not strangers — they are the mind’s own fragments, personified and amplified. The persecutor, the savior, the watcher — all are masks of a self that has become too vast to fit inside its old name. The tragedy of schizophrenia lies not in fragmentation itself, but in the world’s inability to hold such multiplicity. From a neurobiological view, this expansion corresponds to a collapse of neural segregation. Brain networks that should oscillate independently — the default mode, salience, and executive systems — become synchronized in unstable harmony. The machinery of prediction overfits reality; it begins to dream while awake. The schizophrenic brain, in this sense, is not broken but over-connected — a hyperactive web where meaning rebounds endlessly between circuits, never settling. Consciousness becomes echo chamber, infinity reflected within itself. But what psychiatry often overlooks is that within the ruins of psychosis lies the potential for transformation. When the storm subsides, when medication and time restore a fragile coherence, many survivors speak of a strange clarity — as if they have seen the backstage of existence. They return with a knowledge that cannot be taught: that reality is not fixed, that the mind is capable of infinite architectures. They are haunted, yes, but also initiated. They have crossed the frontier between self and cosmos and returned changed. The therapeutic challenge is to translate this initiation into integration. The task is not to deny the visions, but to domesticate them — to weave their symbolic language into personal narrative. Each hallucination contains data about the psyche’s architecture; each delusion, a distorted truth about its yearning. When approached with respect, these fragments become clues to the inner universe that generated them. The therapist becomes archaeologist, reconstructing a broken cathedral from scattered glass. Philosophically, schizophrenia exposes the existential condition that underlies all consciousness: that the self is not a thing, but a fragile process — a balance between differentiation and unity. When that balance breaks, we glimpse what lies beneath individuality: a vast, impersonal field of awareness that holds everything yet belongs to no one. For the schizophrenic, that field is not a mystical abstraction — it is daily experience. The dissolution of boundaries they endure is the metaphysical truth the rest of us only approach through meditation or art: that the mind is the universe looking at itself. And yet, this revelation is unbearable without containment. The mystic and the schizophrenic walk the same road, but one returns while the other remains lost. What separates awakening from psychosis is not content but structure — the ability to anchor infinity in language, body, and relationship. The psychiatrist, then, becomes a builder of bridges: between chaos and coherence, between vision and voice, between cosmos and human form. In this light, schizophrenia is not the negation of meaning but its overflow. The cure is not to extinguish that overflow, but to give it rhythm — to teach the mind to breathe again between its infinities. Medication may quiet the storm, but meaning must be rebuilt by hand, in silence, in dialogue, in art. Many survivors find healing not through forgetting but through creation: painting, writing, composing, transforming their inner multiplicity into beauty. In art, the fragments find order without losing their depth. The self becomes polyphonic, not pathological. Ultimately, schizophrenia reminds us that consciousness is not a stable structure but a fragile miracle of balance. The same mechanism that allows us to imagine, to empathize, to dream — when overstimulated, it shatters. The line between genius and madness, mysticism and psychosis, sanity and dissolution, is not moral but metabolic. To understand schizophrenia is to understand the cost of being human: that to think is to risk breaking the world that thinking creates. At the end of this descent, something remains — not the old self, but a new awareness. It is quieter, humbler, more spacious. The patient learns that coherence is
Schizophrenia and the Shattered Architecture of Reality
There are minds that do not merely suffer — they split.Not into madness, but into multiplicity — into too many selves observing the same world from incompatible angles. Schizophrenia is not only a disease of perception; it is a disturbance in ontology, a fracture in the contract between consciousness and reality. The schizophrenic does not lose touch with the world — the world loses coherence in their touch. In ordinary consciousness, the self acts as a lens through which the world is held together: sensations, thoughts, and emotions converge into one continuous perspective. In schizophrenia, this lens cracks. What was once seamless becomes plural. Thought detaches from thinker, perception detaches from presence. The individual becomes witness to their own mind, hearing it speak in foreign voices. The ego, once the silent conductor of experience, becomes one of the instruments — out of tune, out of order. Neuroscience describes this as a dysregulation of dopamine, a disruption in predictive coding — the brain’s failure to distinguish between internally generated and externally caused stimuli. But this explanation touches only the surface. Beneath the neurochemistry lies something more profound: a crisis in the structure of meaning itself. Schizophrenia reveals the fragility of the boundary that keeps thought private, emotion internal, and the world external. When that boundary dissolves, reality becomes porous — everything speaks, everything connects. The mind perceives infinite pattern where others see randomness. It is not delusion in the simple sense; it is over-meaning, the unbearable saturation of significance. To the schizophrenic, the universe is not silent — it whispers through signs, coincidences, numbers, fragments. Every event becomes message; every gaze, a code. This hyper-symbolic perception, while terrifying, is also profoundly poetic. It is the collapse of ordinary distance between mind and cosmos. The self no longer lives in the world — it is the world, mirrored endlessly through hallucination. Madness, in this light, is not emptiness but overflow. Psychiatry has long struggled with this paradox. How can one heal a consciousness whose illness is the very way it constructs reality? Antipsychotics calm the storm, dampen dopamine, re-stabilize pattern recognition. Yet what they often silence is not only suffering but a strange form of metaphysical creativity — the mind’s attempt to reassemble a fragmented universe. Many patients describe medication not as cure but as narrowing — a return to the smaller world everyone else calls normal. To them, normality can feel like exile from a larger, though dangerous, dimension. From a phenomenological view, schizophrenia is not merely the breakdown of cognition but the expansion of ontological permeability. The barriers between thought and world, subject and object, dissolve. Heidegger called this “unconcealment without control” — the raw exposure of Being without the filter of selfhood. The schizophrenic does not interpret reality incorrectly; they experience too much of it, all at once, without hierarchy. They are like a radio receiving every frequency simultaneously, unable to tune out the noise of existence. The tragedy lies not in their distance from reality, but in their unbearable intimacy with it. Culturally, schizophrenia is the mirror of modernity. In a society where identity is fragmented, communication overloaded, and meaning unstable, the schizophrenic mind embodies the collective condition in extreme form. We live in an era of hallucinated realities — digital selves, algorithmic voices, invisible surveillance. The boundaries of the self dissolve daily into virtuality. Perhaps schizophrenia is not an exception but a revelation — the psyche’s prophetic reflection of what humanity is becoming. Yet within the depths of this fracture, there is something sacred. Many who have survived psychosis describe moments of terrifying beauty — an experience of cosmic unity, an ecstatic fusion of mind and universe. What psychiatry labels delusion can, in certain contexts, resemble mystical vision. The difference lies not in content but in containment. The mystic returns from the vision; the psychotic drowns in it. One integrates the infinite; the other is consumed by it. Both, however, touch the same ocean of consciousness. Therapeutically, true care requires more than suppression. The psychiatrist must stand as both scientist and witness, holding the patient between chaos and coherence. The goal is not to erase the visionary world but to help the patient anchor within it — to translate infinite significance into manageable meaning. Psychotherapy becomes the art of re-threading narrative, rebuilding the fragile membrane that allows a self to exist amid infinity. Neuroscience, meanwhile, is beginning to glimpse the biological mirror of this process. Research into cortical connectivity suggests that psychosis involves excessive synchrony — networks that should oscillate separately become entrained, producing cross-talk between imagination and perception. The brain loses its modularity; dreams leak into waking life. In this sense, schizophrenia may represent consciousness turned inward too far — the dream factory overriding the sensory gate. Treatment, then, is not merely pharmacological correction but the re-establishment of rhythmic distinction between world and self. And yet, to speak of schizophrenia only as dysfunction misses its existential significance. It reveals something essential about being human: that reality itself depends on a fragile act of trust. We believe our thoughts are our own, our senses reliable, our world shared. Schizophrenia exposes this faith as a construction — delicate, provisional, and astonishingly brave. Those who fall through its cracks show us the invisible scaffolding of sanity. Perhaps one day, psychiatry will no longer see schizophrenia solely as pathology, but as a radical form of consciousness — a painful experiment in what it means to exist without walls. Such a view does not romanticize suffering; it recognizes the depth from which it arises. The schizophrenic is not lost outside reality but submerged within it, trapped in a flood of meanings the rest of us have learned to ignore. Healing, therefore, means learning to navigate infinity without drowning. At the far end of recovery, some patients describe an unexpected peace — not the return to who they were, but the acceptance of what they have become: witnesses to the porousness of reality. They move carefully through the world, aware that
Emptiness as the Final Frontier of Consciousness
Emptiness, once seen as an affliction, reveals itself at last as a horizon — not a void to be crossed but a depth to be understood. The patient who has endured the slow erosion of meaning eventually begins to perceive something subtle beneath the silence: a pulse, a presence without name. This is not the return of emotion as it once was; it is the first whisper of existence becoming aware of itself again. Out of nothing, consciousness begins to weave the faint threads of new meaning. The transformation does not occur through will or logic. It happens quietly, in the hidden spaces between despair and surrender. When the self stops trying to rebuild its old architecture, a new form of being begins to arise — not constructed but discovered. The emptiness that once felt like death now becomes transparent, and through it, life glows in its rawest form. The individual realizes that what they called “nothing” was never absence at all; it was pure potential, unshaped and infinite. Psychiatry, standing at the edge of this revelation, faces a paradigm shift. Its tools — neuroimaging, pharmacology, psychotherapy — can touch the surface of emptiness but not its essence. For the void is not a neural dysfunction; it is consciousness in transition. The brain, that intricate instrument of perception, undergoes a kind of quantum reorganization when meaning collapses. Default patterns of thought and emotion dissolve, making space for a new order — not imposed, but emergent. The process mirrors what physicists describe in the universe: chaos preceding new form, entropy preceding creation. In this sense, the psyche is cosmological — a small universe learning to reinvent itself. Those who have passed through the Emptiness Syndrome often speak of an after-state that defies diagnosis. They describe an unexpected peace, not of happiness but of transparency. They still see the same world, yet it appears weightless, luminous, somehow realer than before. Objects no longer carry the heavy demand to signify; they simply are. Emotions no longer chain them; they move freely, like clouds. What once felt like detachment now becomes clarity. The mind no longer clings — it observes, participates, and releases. It has learned the art of lightness without loss. In this new consciousness, meaning is not something to be found but something that flows through presence itself. Every act — breathing, speaking, touching — becomes a small creation of significance. There is no longer the old dichotomy of purpose and purposelessness; there is only participation. The individual no longer asks, “Why do I exist?” but rather, “How can I fully exist in this moment?” This subtle shift marks the end of existential anxiety. The void remains, but it has become friendly. Neuropsychologically, this shift corresponds to a rebalancing between the brain’s default mode network and its task-positive systems — between self-referential rumination and direct engagement. The self that once looped endlessly in internal reflection now rests in dynamic equilibrium with the world. The sense of “I” becomes fluid, relational, grounded not in thought but in awareness itself. The psychiatric implication is profound: healing does not mean returning to one’s former identity but learning to exist without needing one. Culturally, this awakening challenges the very foundation of modern identity. The capitalist psyche thrives on lack — the endless hunger for more: more achievement, more validation, more self. But those who have touched true emptiness discover that fulfillment does not come from addition but subtraction. The richest state of mind is not abundance but simplicity. A society built on constant stimulation will find this truth almost unbearable — for silence cannot be monetized, and presence cannot be marketed. Yet it is precisely this silence that our age most desperately needs. Spiritually, emptiness becomes revelation. The mystics have said for millennia what neuroscience is only beginning to confirm: that the core of consciousness is void, but that void is luminous. The Buddhists call it śūnyatā, the mystics union, the poets grace. All point to the same realization — that to lose oneself completely is to discover the one self that never leaves. In this state, there is no boundary between self and other, subject and object, therapist and patient. The psychiatrist who accompanies such a journey no longer treats illness but witnesses awakening. The consulting room becomes a sacred space where two awarenesses dissolve into one shared silence. At the deepest level, emptiness teaches that consciousness is self-generating. Meaning is not something added to existence; it is existence perceiving itself through form. Every mind is thus a mirror in which the universe contemplates its own unfolding. To encounter nothingness is to see through the illusion of separation — to understand that the suffering of emptiness was never punishment, but preparation. The soul empties itself so that it can hold infinity. This understanding reshapes psychiatry’s ethical foundation. No longer can healing be defined merely as the restoration of function or normality. True healing means awakening — helping the mind remember its own depth. The psychiatrist’s role, in this new paradigm, is not only to cure but to accompany: to stand beside another consciousness as it traverses its inner cosmos. The tools of medicine remain vital, but they serve a greater end — the expansion of awareness itself. Psychiatry thus becomes the art of conscious evolution. And so, the story comes full circle. What began as pathology ends as philosophy. The patient who once whispered, “I feel nothing,” becomes the one who can finally say, “I feel everything, and I am at peace.” Emptiness reveals itself as the mother of meaning, the silent origin of all experience. The void that once terrified now feels like home.

The Anatomy of Nothingness
Emptiness is not the absence of experience; it is the experience of absence. It is the silent scream of consciousness when every structure of meaning has dissolved but awareness remains intact. Patients who live within this condition are not broken — they are suspended. They inhabit a state where perception continues but participation fails. It is not pain that torments them, but the unbearable neutrality of existence. They are neither fully alive nor dead, caught in the liminal zone between being and non-being. To understand this condition, psychiatry must leave the comfort of diagnosis and enter metaphysics. Emptiness is not merely a symptom; it is a mode of existence — an ontological configuration of the mind. Beneath its psychological surface lies a profound tension between awareness and attachment. The human psyche cannot live on awareness alone; it needs form, narrative, desire — it needs something to lean on. When those attachments dissolve — through trauma, disillusionment, or the collapse of identity — awareness remains, naked and unanchored. This raw consciousness perceives everything yet touches nothing. It is both infinite and unbearable. Neuroscience offers a glimpse into this inner desert. Studies on depersonalization and derealization reveal disruptions in the insula, the brain region that integrates bodily sensation with emotional salience. Without this integration, perception loses its warmth. The world becomes visually intact but emotionally dead — a simulation without depth. In emptiness, the self is not destroyed but disconnected from its own embodiment. The mind floats above the flesh, observing without feeling. It is as if the soul has become a spectator of its own life. But what modern neuroimaging cannot capture is the metaphysical terror of this state — the existential vertigo of realizing that nothing inside truly responds. This is where psychiatry touches philosophy again. Emptiness is consciousness stripped of illusion. It exposes the scaffolding of selfhood and the artificiality of meaning. Most humans live buffered by the soft hallucinations of purpose, love, and identity. When those dissolve, what remains is not madness — it is truth, raw and silent. But few can endure that truth without disintegration. Thus, the mind invents symptoms to fill the void: anxiety, compulsion, obsession — each an attempt to restore texture to the flatness of being. Culture amplifies this pathology. The modern subject is defined not by interiority but by exposure. To exist is to be seen; to feel is to perform. The social media mirror multiplies the self until it becomes translucent. In the endless reflection of images, the soul evaporates. Loneliness becomes hyper-visible but intimacy becomes impossible. The body becomes content; emotion becomes currency. Under such conditions, emptiness is not a disorder — it is the logical outcome of existing without depth. The psyche collapses under the weight of its own simulation. Yet emptiness is not the end of meaning — it is the clearing where new meaning can emerge. Those who endure it without fleeing discover that nothingness is not sterile. It is fertile in its silence. When stripped of artificial structure, the psyche begins to generate authenticity from within. This process is painful and slow, but it is the foundation of transformation. The void becomes a womb. In its darkness, the self reorganizes around direct experience rather than borrowed identity. What once felt like death reveals itself as birth in disguise. Therapeutically, the psychiatrist must resist the impulse to fill the void too quickly. Medication may soothe the body, but the deeper cure is existential courage — the willingness to remain conscious inside the emptiness. The therapist’s presence becomes a mirror in which the patient learns that the void can be inhabited, not escaped. Healing begins when the patient realizes that the emptiness is not a defect but a doorway. In this sense, therapy becomes an act of ontological companionship — two consciousnesses facing the silence together until it begins to speak. The spiritual traditions of East and West have long known this terrain. In Zen, the moment of kenshō — seeing one’s true nature — often follows the collapse of meaning. The practitioner falls into the abyss of nothingness only to realize that it is made of light. Similarly, in Christian mysticism, the “dark night of the soul” precedes union with the divine. Both traditions describe what psychiatry now rediscovers through the language of neuroplasticity and consciousness studies: that the death of false meaning is the beginning of real awareness. From a biological standpoint, the return from emptiness corresponds to the reactivation of affective circuits — particularly those linking the insula, anterior cingulate, and limbic structures. But this reactivation cannot be forced; it must be invited through experience. Meaning, in the brain, is not a cognitive event but an embodied rhythm — the re-synchronization of thought and feeling, self and world. Thus, recovery from emptiness is not achieved by understanding it intellectually, but by re-learning to feel safely. The goal is not to escape the void, but to dance within it. Philosophically, emptiness reveals the most fundamental paradox of consciousness: that the ground of being is also the absence of form. The universe itself is born from nothing, yet that nothing sustains everything. The psyche mirrors this cosmology. Beneath every thought, memory, and desire lies a silent field of awareness — vast, empty, and eternal. To encounter emptiness, then, is to meet the origin of the self. It is terrifying because it dissolves all distinctions, but liberating because it shows that one was never truly separate. The ego dies, but life continues. Perhaps psychiatry’s greatest task in the coming century will be to integrate this realization — to evolve from a science of dysfunction into a science of consciousness. The future psychiatrist will not only treat disorders of mood or perception but guide human beings through the thresholds of awareness itself. Emptiness, once feared as a void, will be recognized as a dimension of reality — a necessary phase in the evolution of mind. Suffering will no longer be viewed solely as pathology, but as initiation: the