Anxiety, in its clinical form, is classified as a mental disorder that can significantly impair daily functioning. However, when examined on a broader psychological spectrum, anxiety reveals itself as a nearly universal human condition. Subclinical anxiety—defined as persistent anxious thoughts and physiological responses that do not meet diagnostic thresholds—can be observed in an overwhelming majority of individuals. While not pathological in itself, this condition quietly shapes perception, decision-making, and emotional regulation in almost every human life. https://youtu.be/tni2IXgPAt4?si=u7qIqUhx_qFLIuDj From an evolutionary standpoint, anxiety emerged as an adaptive mechanism. The human brain evolved to detect threats rapidly, prioritize negative information, and anticipate potential dangers. These cognitive tendencies, while essential for survival in hostile environments, remain active in modern contexts where threats are largely abstract or symbolic. As a result, individuals frequently experience excessive worry about social evaluation, future uncertainty, productivity, or personal adequacy. Such concerns, though normalized and socially reinforced, represent core components of subclinical anxiety. One of the defining characteristics of this condition is cognitive hypervigilance—a heightened sensitivity to potential problems, mistakes, or rejection. People often replay past interactions, catastrophize minor setbacks, or mentally rehearse future scenarios in an attempt to maintain control. This constant mental scanning is rarely recognized as a psychological issue because it is so widespread. Yet research in cognitive psychology demonstrates that chronic worry consumes attentional resources, diminishes working memory capacity, and contributes to emotional fatigue. Another pervasive feature is somatic anxiety, which manifests through bodily sensations such as muscle tension, accelerated heartbeat, shallow breathing, or gastrointestinal discomfort. Many individuals interpret these sensations as normal stress responses without acknowledging their psychological origin. Over time, the body becomes conditioned to remain in a state of low-grade arousal, blurring the boundary between normal functioning and persistent physiological stress. Importantly, subclinical anxiety is reinforced by contemporary social structures. Digital connectivity, performance-based education systems, economic instability, and constant comparison through social media intensify self-monitoring and fear of inadequacy. In such an environment, anxious cognition is not only common but often rewarded, as vigilance and over-preparation are mistaken for responsibility or ambition. Despite its prevalence, subclinical anxiety is frequently dismissed because it does not disrupt external functioning. Individuals continue to work, study, and socialize, while internally navigating relentless mental pressure. This invisibility contributes to the misconception that psychological well-being is binary—either disordered or healthy—when in reality it exists on a continuum. The danger lies not in anxiety itself, but in its normalization to the point where chronic psychological strain is considered an inevitable aspect of being human. Addressing this condition does not necessarily require clinical intervention. Awareness, emotional literacy, mindfulness-based practices, and cognitive restructuring can significantly reduce its impact. Recognizing that constant worry is not a personal failure but a shared psychological pattern allows individuals to relate to their mental experiences with greater compassion and critical distance. In conclusion, subclinical anxiety represents a psychological condition whose traits are present in the vast majority of people. While it may never be formally diagnosed in most cases, its influence on mental health, cognition, and quality of life is profound. Understanding its universality is a crucial step toward redefining mental health not as the absence of symptoms, but as the capacity to coexist with the mind’s inherent tendencies without being governed by them.

Silent Reversibility Reconstruction
After the Post-Irreversible Adaptation Void, some individuals enter a phase that is almost never recognized as recovery, because it does not feel like recovery at all. This stage, which can be called Silent Reversibility Reconstruction, is defined not by relief, insight, or emotional return, but by something far quieter: the gradual reappearance of change itself, unnoticed and unobserved. The defining feature of this phase is that nothing dramatic happens. There is no moment of “coming back,” no emotional breakthrough, no realization that the crisis is over. In fact, individuals who closely monitor themselves often believe that nothing is improving. Yet beneath conscious awareness, the mind begins to tolerate transitions again. States shift without triggering alarm. Thoughts arise and pass without being checked for permanence. This happens not because the person trusts reversibility, but because the mind stops asking whether reversibility exists. Phenomenologically, experience regains micro-mobility. Small variations in mood, attention, and energy occur without being framed as threats. The present moment no longer feels hardened or final; it becomes slightly porous. Importantly, this porosity is not perceived as safety—it is perceived as normality, which is why it is easy to miss. Patients often report, in retrospect, that they were already improving before they realized improvement was possible. This stage differs sharply from insight-based recovery. Understanding what happened, naming the condition, or making sense of the past may still feel impossible or even dangerous. But meaning is no longer required for stabilization. The nervous system relearns what the mind cannot yet believe: that internal states change on their own. This learning is procedural, not conceptual. A key characteristic of Silent Reversibility Reconstruction is the return of unmonitored engagement. The individual becomes absorbed in tasks without checking how they feel during them. Time passes without being measured. Conversations end without post-analysis. These moments are brief at first and often dismissed as irrelevant, yet they are structurally decisive. Each unmonitored transition weakens the memory of irreversibility. Neuropsychologically, this phase likely reflects the reactivation of state-switching mechanisms that were suppressed during existential threat. Once the brain no longer treats internal change as catastrophic, it allows variability again. However, because this occurs below reflective awareness, attempts to observe or accelerate the process can interfere with it. The mind that watches too closely reintroduces rigidity. Clinically, this phase is often misunderstood or interrupted. Patients may return to therapy seeking the “return of self,” only to be confused when no such moment arrives. Clinicians may push for emotional exploration or narrative integration too early, inadvertently pulling the person back into monitoring. In some cases, improvement stalls not because recovery is impossible, but because it is being demanded to appear. The risk in this stage is subtle: impatience. The individual may conclude that this muted functioning is the final form of life, unaware that flexibility is already reassembling itself in the background. Conversely, fear of relapse may cause avoidance of novelty, slowing the reconstruction process. What is required instead is tolerance of ambiguity—living without confirming whether one has returned. Silent Reversibility Reconstruction reveals a counterintuitive truth: the mind does not regain reversibility by proving that return is possible. It regains it by forgetting to ask. Recovery, here, is not a destination but a fading of vigilance—a disappearance of the very question that once dominated consciousness. This stage marks the point at which the psyche quietly resumes its most fundamental capacity: to move, to shift, and to leave states without ceremony. Not everything comes back, and not everything needs to. What returns first is not identity or emotion, but flow. And in that flow, life begins again—without announcing that it has done so.

Post-Irreversible Adaptation Void
After intense Irreversibility Anxiety, some individuals do not return to their previous mental state, yet they also do not deteriorate into psychosis or collapse. Instead, they enter a little-described psychological phase that can be called Post-Irreversible Adaptation Void. This state emerges not at the peak of fear, but after the mind realizes—often with surprise—that it has continued functioning despite the conviction that return was impossible. In this phase, the acute terror has faded, but relief does not arrive. The individual no longer feels trapped in panic, yet does not feel restored either. The defining feature is a void-like neutrality: the sense that something fundamental ended, but nothing clearly replaced it. Patients often say, “I survived it, but I don’t know what I survived,” or “I’m functioning, but I don’t feel re-entered into life.” Unlike depression, the void is not characterized by sadness, hopelessness, or self-criticism. Energy may be adequate, sleep may normalize, and cognitive clarity often improves. The problem is subtler: the old sense of psychological elasticity—the trust that one can fully inhabit states and then leave them—has not yet returned. Life feels navigable but strangely non-immersive, as if the mind is operating in a post-event mode without a clear narrative of what changed. Phenomenologically, this state involves a thinning of existential intensity. Experiences register, decisions are made, conversations occur, but with reduced depth. This is not emotional numbing in the classic sense; emotions can occur, but they feel provisional, as if they are being tested rather than inhabited. The individual may fear that this flattened mode is permanent, yet the fear itself lacks urgency, creating a quiet, unsettling ambiguity. This condition differs from depersonalization in an important way. In depersonalization, the self feels unreal or detached. In the Post-Irreversible Adaptation Void, the self feels real but post-traumatic, even when no external trauma occurred. The trauma was internal and structural: the confrontation with perceived irreversibility. The psyche reorganized itself to survive that confrontation, but has not yet reintegrated flexibility. Neuropsychologically, this phase may represent a protective stabilization. After extreme existential threat, the brain may reduce intensity to prevent reactivation of catastrophic fear. This creates a buffer zone—safe, functional, but experientially muted. Clinically, this is often mistaken for recovery or dismissed as residual anxiety, causing patients to feel unseen. They know something is different, but lack language to describe it. A critical risk in this phase is premature forcing of “normality.” When individuals push themselves to feel the way they did before—seeking emotional intensity, insight, or existential certainty—the void may deepen or reactivate irreversibility fears. Conversely, passive resignation can cause the state to solidify. The challenge lies in allowing gradual re-engagement without demanding restoration. Therapeutically, the task is not reassurance or interpretation, but re-flexibilization. Gentle exposure to change—shifts in routine, environment, bodily states—can slowly rebuild trust in psychological movement. Importantly, the individual must experience change without monitoring it. Recovery here is not an insight, but a series of unnoticed transitions that re-teach the nervous system that states evolve on their own. The Post-Irreversible Adaptation Void reveals a rarely acknowledged truth: surviving a perceived point of no return does not immediately restore the sense of return. The mind may live on before it knows how to live back. This phase is not pathology in the traditional sense, but a transitional ecology of consciousness—quiet, uncertain, and deeply human. Understanding this state challenges psychiatry to recognize not only breakdown and recovery, but the fragile psychological terrain in between, where the mind is no longer collapsing, yet has not learned how to flow again.

Irreversibility Anxiety
Human psychological stability depends not only on memory, identity, or emotion, but on a largely invisible assumption: the belief that one can return. Return to a previous mental state, return to normality, return to oneself. In Irreversibility Anxiety, this assumption collapses. The individual becomes haunted not by what is happening, but by the felt certainty that what is happening cannot be undone. Irreversibility Anxiety is not simply fear of permanence or aging, nor is it equivalent to catastrophic thinking. It is a deep, pre-reflective disturbance in which the mind loses confidence in its own reversibility. Patients often describe the experience as “crossing a line,” “going too far,” or “having seen something that cannot be unseen.” Importantly, this sense of irreversibility may arise without any dramatic external event. A thought, realization, altered state, or subtle shift in consciousness can be enough to trigger it. Unlike panic disorder, where fear peaks and resolves, Irreversibility Anxiety is sustained and existential. The anxiety does not ask, “What if something bad happens?” but rather, “What if I am already past the point of return?” The distress is not about future consequences, but about a perceived loss of psychological undo-function. The person may remain fully rational, oriented, and articulate, yet feel trapped in a state that feels qualitatively final. Phenomenologically, this condition is marked by a collapse of temporal elasticity. Normally, mental states are experienced as fluid and revisable. In Irreversibility Anxiety, the present hardens. Thoughts and perceptions feel locked in place, as if consciousness itself has become brittle. This can lead to hyper-monitoring of mental states, as the individual constantly checks whether they are “back yet,” paradoxically reinforcing the sense that return is impossible. This phenomenon differs from depersonalization and derealization. In those conditions, experience feels unreal or distant. In Irreversibility Anxiety, experience feels too real, too fixed. The problem is not detachment, but entrapment. The self feels fully present but unable to retreat. Patients may say, “I am still me, but I can’t step away from this version of me.” Neurocognitively, Irreversibility Anxiety may involve dysfunction in neural systems responsible for contextual updating and state-switching. The brain normally signals that internal states are temporary. When this signaling weakens, transient experiences are misclassified as permanent transformations. This misclassification generates intense fear, even when no objective deterioration is occurring. Behaviorally, individuals may seek reassurance compulsively—asking whether others have recovered from similar states, rereading past memories to confirm continuity, or testing emotions repeatedly to see if change is still possible. Others may avoid introspection entirely, fearing that further self-observation will deepen the sense of irreversibility. Both strategies tend to fail, as the core disturbance lies beneath conscious control. Clinically, Irreversibility Anxiety is often misunderstood as obsession, generalized anxiety, or early psychosis. Yet it does not center on content, belief, or fear of harm. Its object is structural: the perceived loss of mental reversibility itself. This makes standard reassurance ineffective. Telling the patient “this will pass” often fails, because the capacity to believe that things pass is precisely what has been compromised. Therapeutic approaches remain tentative. Interventions that emphasize time, rhythm, and physiological state-shifting may be more effective than insight or reassurance. Sleep, bodily regulation, and non-reflective engagement can gradually restore the felt sense that states change without requiring proof. The goal is not to convince the mind that return is possible, but to allow the nervous system to experience change directly. Irreversibility Anxiety reveals a fragile foundation of mental health: the implicit belief that consciousness is reversible. When this belief collapses, suffering emerges even in the absence of delusion, mood disorder, or cognitive impairment. The condition suggests that one of the mind’s deepest needs is not control or meaning, but the quiet assurance that no mental state is final.
Existential Motor Inhibition
In psychiatry, motor inhibition is usually associated with depression, catatonia, or neurological disease. Patients move slowly, speak less, or appear physically constrained. Far less recognized is a condition in which physical movement remains intact, cognition remains clear, and motivation is not consciously absent—yet the fundamental capacity to initiate existence feels impaired. This phenomenon can be described as Existential Motor Inhibition, a state in which the individual can act, but cannot naturally begin. Individuals experiencing existential motor inhibition often report that nothing feels impossible, yet nothing truly starts. They can get out of bed, speak, work, and respond when required, but spontaneous action feels inaccessible. Life becomes reactive rather than generative. The person waits—not for motivation, pleasure, or meaning—but for an internal “go-signal” that never arrives. This waiting is not passive; it is tense, effortful, and exhausting. This condition differs from depression in crucial ways. There may be no sadness, guilt, hopelessness, or negative self-concept. Energy levels can be normal, and sleep and appetite may be intact. Unlike avolition, the person does not lack desire; they may want to act intensely. What is missing is the implicit sense of permission to begin. Patients often say things like, “I can do things once I’m already doing them, but starting feels blocked,” or “Life feels paused, but not empty.” Phenomenologically, existential motor inhibition is experienced as a disruption in temporal agency. Normally, the self experiences itself as flowing naturally into the next action. In this state, that flow fractures. Each action must be consciously forced across a gap that should not be there. This creates a peculiar form of fatigue: not from effort itself, but from repeatedly overcoming an invisible threshold. Cognitively, individuals often remain sharp and self-aware. They can analyze their condition accurately and may even describe it with remarkable precision. This insight, however, does not restore agency. Unlike anxiety disorders, the inhibition is not driven by fear of outcomes. Unlike obsessive–compulsive disorder, it is not driven by doubt. The blockage feels pre-cognitive, as if the mechanism that translates intention into initiation has gone offline. Neuropsychologically, this phenomenon may involve dysfunction in systems responsible for action initiation rather than action planning or execution. The brain may still generate goals and evaluate options, but the signal that normally tips intention into movement fails to fire reliably. Because the person can still act under external structure—deadlines, instructions, emergencies—the condition is often invisible to others and deeply isolating to the sufferer. Over time, existential motor inhibition can erode identity. The individual may begin to feel less like an agent and more like an object being moved by circumstances. Relationships suffer not because of emotional withdrawal, but because initiative disappears. Creative individuals often find this state especially distressing, as creativity depends on spontaneous beginning rather than response. Treatment remains poorly defined. Encouragement, insight, or motivation-based interventions often fail, as the problem is not willingness. Forcing productivity may worsen the sense of internal blockage. Some therapeutic approaches focus instead on restoring rhythmic initiation through embodied practices—movement, pacing, repetitive action—rather than meaning or emotion. The aim is to reestablish initiation as a bodily process before it becomes a psychological one. Existential Motor Inhibition exposes a blind spot in psychiatric thinking: the assumption that if someone can act, they can also begin. This condition shows that initiation itself is a fragile psychological function, distinct from desire, energy, or cognition. When it collapses, life does not stop—but it no longer truly starts.
Pre-Delusional Transparency
Psychiatry often conceptualizes psychosis as a break from reality characterized by false beliefs, hallucinations, or disorganized thought. Far less attention is given to a subtle but clinically significant state that can precede delusion without crossing into it. This condition, which may be described as Pre-Delusional Transparency, involves an abnormal increase in the perceived clarity, coherence, and self-evidence of reality itself. Rather than feeling confusing or unreal, the world feels too clear, as if its structure has been exposed. Individuals experiencing this state do not report bizarre beliefs. Instead, they describe a disturbing sense that nothing is hidden anymore. Objects, people, and situations appear stripped of ambiguity. Social interactions feel mechanistic, predictable, and overly legible. The individual may say that they can “see through” situations instantly or that meanings present themselves without effort. Crucially, this clarity is not experienced as insight or relief, but as invasive and destabilizing. This phenomenon differs from paranoia in that there is no persecutory intent attributed to others. It also differs from mania, as there is no grandiosity or elevated mood. Cognitive function often remains sharp, and the individual may even become more articulate. What changes is the epistemic distance between the subject and the world. Normally, reality contains opacity—gaps, uncertainties, and interpretive friction that allow psychological breathing room. In Pre-Delusional Transparency, this opacity collapses. Phenomenologically, the person experiences a loss of interpretive freedom. Meaning no longer feels constructed or negotiable; it feels imposed. Situations announce their significance immediately, leaving no space for doubt or reinterpretation. This can produce intense anxiety, as the mind senses that a fundamental buffer has been removed. Patients often report a fear that this clarity will “lock in” permanently or escalate into something irreversible. Neurocognitively, this state may involve excessive precision weighting in predictive processing systems. The brain begins to over-trust its immediate interpretations, reducing tolerance for uncertainty. Unlike full delusion, however, the individual may still question this process, recognizing that something is wrong with the way meaning is arriving rather than with the content itself. This fragile insight is often what prevents the transition into psychosis. Clinically, Pre-Delusional Transparency is difficult to detect. Patients may sound coherent, insightful, and even philosophical. Without careful phenomenological inquiry, clinicians may overlook the underlying distress and misinterpret the experience as intellectual curiosity or heightened awareness. Yet many patients describe this state as one of the most frightening experiences of their lives, precisely because it feels like the final step before losing interpretive autonomy. Behaviorally, individuals may attempt to reintroduce ambiguity by avoiding eye contact, social situations, or reflective thought. Others may engage in compulsive doubt, deliberately questioning obvious interpretations to restore uncertainty. These strategies can temporarily relieve anxiety but often reinforce hyper-awareness of meaning. Therapeutic intervention at this stage is crucial yet underdeveloped. Confrontational reality testing is unnecessary and potentially harmful, as reality testing is not yet lost. Instead, treatment may focus on restoring epistemic humility—helping the mind relearn that ambiguity is not a threat but a stabilizing feature of experience. Gentle grounding, reduction of cognitive overstimulation, and avoidance of excessive introspection may help preserve the remaining buffer between perception and belief. Pre-Delusional Transparency challenges the assumption that clarity is always healthy. It suggests that mental stability depends not on maximal understanding, but on a delicate balance between knowing and not-knowing. When the world becomes too transparent, the mind risks losing the very uncertainty that protects it from collapse.
Affective Muting with Preserved Cognition
Psychiatric literature often assumes that emotional flattening is accompanied by cognitive decline, psychosis, or neurological damage. However, a rarely examined condition exists in which emotional experience fades or disappears while cognitive clarity, memory, logic, and self-awareness remain largely intact. This phenomenon, which may be described as Affective Muting with Preserved Cognition, represents a profound but poorly categorized form of psychological suffering that does not align cleanly with depression, negative symptoms of schizophrenia, or depersonalization. Individuals experiencing affective muting do not necessarily report sadness, emptiness, or despair. Instead, they describe the absence of emotional signal altogether. Events that would normally evoke pleasure, fear, grief, or attachment register cognitively but fail to generate affective resonance. The person understands that something should feel meaningful, yet nothing arises internally. Unlike anhedonia, which is often specific to pleasure, affective muting extends across the emotional spectrum. Even anxiety and sadness may be inaccessible, leaving the individual in a state of emotionally silent consciousness. What distinguishes this condition from major depressive disorder is the absence of negative affect and self-critical cognition. Thought processes remain organized, reflective, and sometimes even creative. Motivation may persist at a behavioral level, yet actions feel mechanical rather than emotionally driven. Patients often say, “I know what I am doing and why, but I no longer feel why it matters.” This creates a unique form of distress rooted not in pain, but in the loss of emotional reference points that normally guide meaning and decision-making. Phenomenologically, affective muting is often experienced as a loss of internal depth rather than emotional blunting. The world does not feel unreal, as in derealization, nor does the self feel detached, as in depersonalization. Instead, experience feels flattened along the emotional dimension while remaining perceptually and intellectually vivid. This can be deeply disorienting, particularly for individuals who previously relied on emotion to structure identity, relationships, or creativity. Neurobiologically, this state may reflect a selective disruption of limbic signaling or affective integration rather than global dysfunction. Emotional appraisal systems may still identify relevance, but fail to translate that relevance into felt experience. This decoupling between appraisal and affect suggests that emotion is not merely an epiphenomenon of cognition, but a distinct channel of consciousness that can be selectively silenced. Clinically, affective muting is frequently misunderstood or minimized. Because patients do not appear depressed, agitated, or psychotic, their suffering may be dismissed as existential or philosophical. Standard depression scales often fail to capture the condition, as they rely on the presence of negative emotion. Similarly, treatments aimed at mood elevation may prove ineffective or even alienating, as there is no mood to elevate. The psychological consequences are significant. Without emotion, moral intuition, attachment, and future orientation become abstract rather than felt. Relationships may be maintained out of obligation or habit rather than connection. Some individuals describe a sense of being “ethically intact but emotionally absent,” raising complex questions about responsibility, agency, and authenticity in the absence of feeling. Therapeutic approaches to affective muting remain experimental. Insight-based therapy may have limited impact, as understanding is already preserved. Some clinicians report cautious success with interventions that emphasize sensory and affective re-engagement rather than narrative or cognitive restructuring. The aim is not to force emotion, but to create conditions in which affective signals might re-emerge spontaneously. Affective Muting with Preserved Cognition challenges a core assumption in psychiatry: that emotional suffering is defined by the presence of painful feelings. In this condition, suffering arises from their absence. It suggests that mental health depends not only on rational coherence or behavioral function, but on the quiet, often unnoticed presence of emotion as the substrate of human significance.

Temporal Disintegration Anxiety
Psychiatry traditionally treats time distortion as a secondary symptom—something that appears in depression, mania, trauma, or psychosis. Slowed time in melancholia, accelerated time in mania, or frozen time in trauma are well documented. Far less examined, however, is a phenomenon in which time itself becomes the primary object of anxiety. This condition, which may be called Temporal Disintegration Anxiety, arises when an individual loses implicit trust in the continuity, reliability, and coherence of subjective time. Temporal Disintegration Anxiety is not simply fear of the future or regret about the past. Rather, it is a persistent unease that the flow of time is unstable, fragile, or liable to collapse. Patients often describe sensations such as “time feels thin,” “the present doesn’t hold,” or “moments don’t connect properly.” The distress is not tied to a specific event but to the experience of temporality itself. Everyday transitions—finishing a sentence, walking from one room to another, waiting for a response—can provoke subtle panic because the mind no longer assumes seamless continuity between moments. This condition differs from depersonalization and derealization, although overlap exists. In depersonalization, the self feels unreal; in derealization, the world feels unreal. In Temporal Disintegration Anxiety, both self and world may feel intact, yet the bridge between moments feels unreliable. The individual remains oriented, logical, and often highly articulate, but experiences a constant background fear that the present will dissolve before it can stabilize. This creates a state of hyper-attention to “nowness,” which paradoxically disrupts the natural flow of time. Neurocognitively, Temporal Disintegration Anxiety may involve dysfunction in predictive timing mechanisms. The brain normally operates by anticipating the immediate future—milliseconds to seconds ahead—allowing experience to feel continuous. When this predictive buffering weakens, the present becomes effortful rather than automatic. Each moment must be consciously “held together.” This effort is exhausting and often misinterpreted as generalized anxiety or early psychosis, though reality testing typically remains intact. A striking feature of this condition is the patient’s language. Many struggle to describe their distress using conventional emotional terms. Instead, they speak in metaphors of physics or mechanics: slipping, gaps, discontinuities, breaks. Clinicians unfamiliar with phenomenological psychiatry may dismiss these reports as abstract or intellectualized, missing the intense somatic fear beneath them. The anxiety is real, but its object—time itself—is unconventional. Over time, Temporal Disintegration Anxiety can lead to behavioral adaptations that further entrench the problem. Individuals may rely heavily on routines, clocks, recordings, or external markers to reassure themselves that time is moving properly. Others avoid stillness, silence, or unstructured situations where temporal flow becomes more noticeable. Ironically, attempts to control time-awareness often amplify it, reinforcing the sense that time is something that must be monitored. Treatment remains challenging. Purely cognitive approaches often fail because the fear is not propositional; it is pre-reflective. Reassuring the patient that time is continuous does little to restore the felt sense of continuity. Pharmacological interventions may reduce arousal but do not address the core disturbance. Therapeutic approaches that emphasize embodied rhythm—walking, breathing, music, coordinated movement—appear more promising, as they help re-anchor time in the body rather than in abstract monitoring. Temporal Disintegration Anxiety highlights a crucial but neglected dimension of mental health: the human mind does not merely exist in time; it actively constructs time as a lived experience. When that construction becomes unstable, suffering emerges in forms that evade standard diagnostic categories. This phenomenon suggests that some psychiatric distress is not about thoughts, emotions, or identity, but about the very framework that allows experience to unfold. Understanding such conditions may require psychiatry to move beyond symptom checklists and return to careful phenomenological listening—paying attention not only to what patients think or feel, but to how reality itself is structured in their experience.

Narrative Saturation Syndrome
Modern psychiatry places great emphasis on insight, self-reflection, and narrative coherence. Patients are encouraged to understand their past, articulate their emotions, and construct meaningful personal stories. Yet an underrecognized pathological state emerges when this process becomes excessive, rigid, and involuntary—a condition that can be described as Narrative Saturation Syndrome. This phenomenon occurs when the individual’s mental life becomes overfilled with self-explanatory narratives to the point that spontaneous experience, emotional immediacy, and psychological flexibility begin to erode. Narrative Saturation Syndrome is not simply overthinking or rumination. It is characterized by a chronic compulsion to explain oneself internally: why one feels a certain way, what a reaction “means,” how a thought fits into a broader life story, or what psychological mechanism must be responsible. The individual no longer experiences thoughts and emotions as transient mental events but as narrative obligations that must be interpreted, contextualized, and justified. Silence of interpretation becomes intolerable. Every inner state demands a story. Clinically, this condition is most often seen in highly introspective individuals, patients with prolonged exposure to psychotherapy, or those who have extensively consumed psychological or philosophical content. Importantly, intelligence and insight do not protect against it; they may even intensify it. The person may speak fluently about attachment styles, defense mechanisms, trauma models, or cognitive distortions, yet report feeling increasingly distant from authentic experience. Emotional life becomes mediated by explanation rather than lived directly. Unlike depersonalization, where experience feels unreal or detached, Narrative Saturation involves over-reality. Feelings are intensely analyzed but paradoxically less felt. Joy, sadness, anger, or desire are quickly transformed into interpretive objects: “This joy is a defense,” “This sadness is unresolved grief,” “This desire reflects a childhood lack.” Over time, emotional spontaneity collapses under interpretive weight. Patients often describe feeling “psychologically full,” “mentally cluttered,” or unable to encounter the present moment without commentary. From a cognitive perspective, Narrative Saturation may reflect a failure of meta-cognitive inhibition. The mind loses its ability to stop explaining itself. This creates a recursive loop in which awareness observes itself observing itself, generating an infinite regress of self-monitoring. Unlike psychosis, reality testing remains intact. Unlike obsessive–compulsive disorder, the narratives do not feel alien or intrusive; they feel justified, even necessary. This makes the condition difficult to recognize as pathological. The existential cost of Narrative Saturation is significant. Identity becomes rigid rather than flexible. The self is no longer something that evolves implicitly through experience, but a fixed object constantly under review. Many individuals report a sense of being “psychologically trapped inside my own explanation of myself.” This can lead to chronic fatigue, anhedonia, and a subtle despair rooted not in meaninglessness, but in meaning overload. Standard therapeutic approaches can unintentionally worsen this condition. Insight-oriented therapy may reinforce narrative compulsion, while excessive emotional labeling can further distance patients from raw affect. Treatment requires a counterintuitive shift: reducing the centrality of self-explanation. Interventions may focus on cultivating non-narrative modes of experience—physical sensation, action without interpretation, creative expression without analysis. The goal is not to eliminate understanding, but to restore the ability not to understand everything. Narrative Saturation Syndrome exposes a blind spot in contemporary mental health culture. While meaning-making is essential for psychological health, there exists a threshold beyond which meaning becomes oppressive. The mind requires not only coherence, but also silence—spaces where experience is allowed to exist without explanation. When those spaces disappear, the self does not become clearer; it becomes exhausted. This phenomenon suggests a broader implication for psychiatry: psychological suffering can arise not only from confusion or lack of insight, but from an excess of insight that has lost its stopping mechanism. In such cases, healing may involve learning how to let parts of the self remain unexplained.
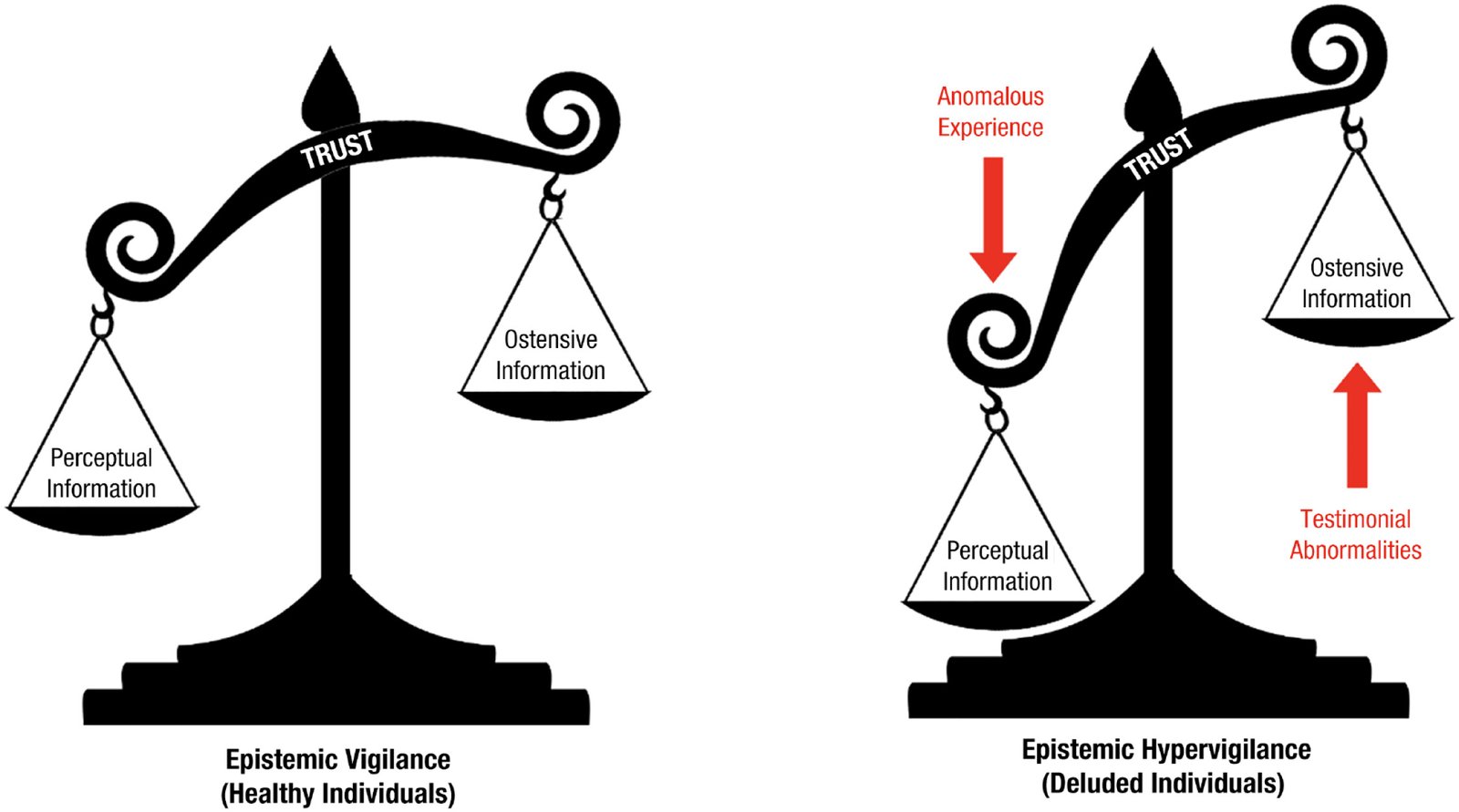
Epistemic Hypervigilance
In classical psychiatry, vigilance is often treated as a neutral or even adaptive cognitive function: the capacity to remain alert to relevant stimuli, detect threats, and update beliefs accordingly. However, a little-examined phenomenon exists at the border between cognition, anxiety, and psychosis, which can be provisionally termed epistemic hypervigilance. This condition is not formally recognized in diagnostic manuals, yet it appears across clinical observations in patients who do not fit neatly into obsessive–compulsive disorder, paranoia, or schizophrenia. Epistemic hypervigilance refers to a persistent, involuntary state in which the mind becomes excessively alert to meaning itself—treating ordinary information, language, coincidence, and internal thoughts as if they carry hidden, urgent, or destabilizing significance. Unlike classic paranoia, epistemic hypervigilance does not necessarily involve fixed persecutory beliefs. Instead, the individual experiences a chronic sense that “something is about to be understood,” “something important is being missed,” or “this detail cannot be random.” The person may remain intellectually skeptical and even insight-oriented, yet is unable to disengage from constant interpretive scanning. Everyday stimuli—phrases overheard in conversation, repeated numbers, subtle changes in tone, minor bodily sensations—are experienced as epistemically charged, as if they demand interpretation. This creates a paradoxical mental state: the subject doubts their interpretations while simultaneously being unable to stop generating them. Clinically, epistemic hypervigilance differs from obsessive rumination. Obsessions are typically recognized as intrusive and irrational, whereas hypervigilant meaning-search often feels compulsively rational. The individual may report that their mind is “over-working,” “connecting too much,” or “refusing to leave things unresolved.” Importantly, this is not merely curiosity or philosophical reflection; it is experienced as exhausting, destabilizing, and often frightening. Patients frequently describe a loss of cognitive rest, as if the mind has lost its capacity for epistemic trust—the basic assumption that most things do not require deep interpretation. Neurophenomenologically, this state may involve dysregulation in salience attribution systems, particularly dopaminergic circuits implicated in assigning importance to stimuli. When salience becomes uncoupled from actual relevance, the mind begins to over-tag neutral events as meaningful. Unlike full psychosis, however, reality testing may remain partially intact. The individual senses that the meaning overload is internal, yet cannot prevent it. This intermediate zone may explain why epistemic hypervigilance is often misdiagnosed as anxiety, high intelligence, or early psychosis depending on the clinician’s framework. One of the most overlooked consequences of epistemic hypervigilance is its impact on identity. Because meaning-making is central to self-narrative, excessive interpretive activity can fragment the sense of self. Patients may report feeling “mentally exposed,” “too conscious,” or unable to return to a previous, more automatic way of being. Over time, this can lead to depersonalization, existential distress, and secondary depression—not because life lacks meaning, but because meaning has become oppressive. Treatment remains largely exploratory. Standard antipsychotics may reduce salience intensity but risk blunting cognition excessively. Cognitive-behavioral approaches often fail because the problem is not faulty beliefs, but an overactive epistemic engine. Some emerging therapeutic strategies focus instead on restoring epistemic trust: helping patients relearn that uncertainty can be tolerated and that not all stimuli require interpretation. Mindfulness-based interventions, when carefully adapted, may help by shifting attention away from meaning extraction toward raw perception, though they can initially worsen symptoms if introduced too abruptly. Epistemic hypervigilance challenges psychiatry’s traditional categories. It raises a deeper question: can the drive to understand reality itself become pathological, not because it is delusional, but because it is unrelenting? As psychiatry increasingly engages with predictive processing and Bayesian models of the mind, this phenomenon may offer a crucial insight—mental illness does not always arise from false beliefs, but sometimes from an inability to stop asking what something means.