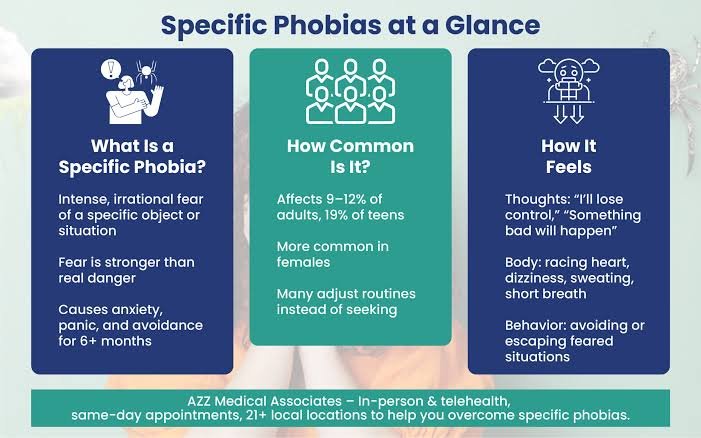
A phobia is far more than an ordinary fear. Nearly everyone experiences fear when confronted with genuine danger, but individuals with phobias develop intense anxiety in response to situations or objects that pose little or no objective threat. A harmless spider, a crowded elevator, an airplane, a needle, or even an open public space may provoke overwhelming panic. Despite recognizing that their fear is excessive, many individuals remain unable to control it. This apparent contradiction has made phobias one of the most fascinating subjects in psychiatry and neuroscience: why does the brain continue producing powerful fear even when logic clearly indicates safety?
For many years, phobias were viewed primarily as learned emotional reactions.
Although learning remains important, modern neuroscience demonstrates that phobias emerge through complex interactions among genetics, brain development, emotional regulation, memory, attention, and evolutionary survival mechanisms.
Fear itself is not pathological.
It is an adaptive biological response that has protected humans throughout evolution.
Without fear, survival would have been impossible.
The challenge arises when this protective system begins responding to harmless situations as though they represent life-threatening danger.
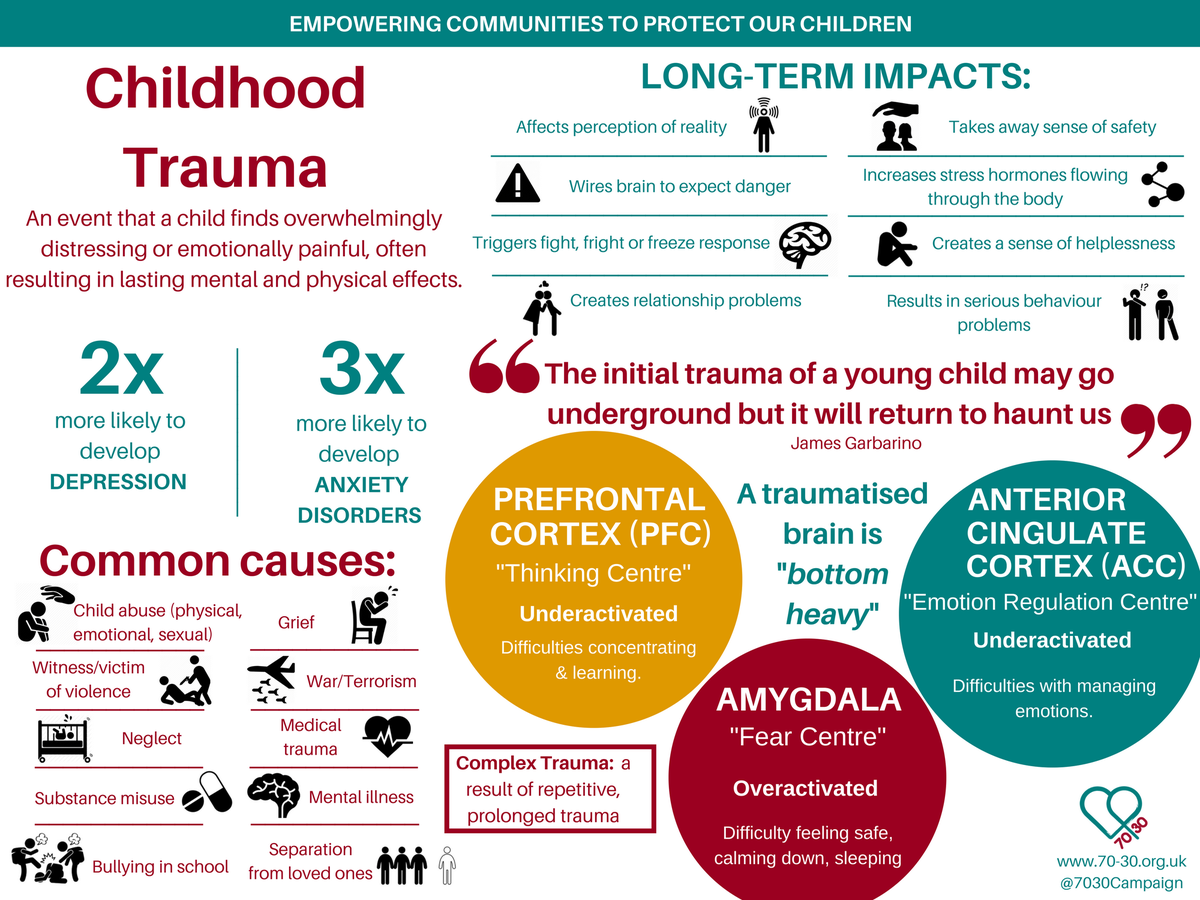
The amygdala plays a central role in this process.
Rather than functioning simply as a “fear center,” the amygdala continuously evaluates the emotional significance of incoming information.
Its primary task is rapid threat detection.
Importantly, the amygdala responds before conscious reasoning has fully evaluated the situation.
This explains why individuals often experience fear before they have time to think logically.
The emotional reaction precedes conscious interpretation.
Evolution favored this arrangement because reacting too quickly occasionally was safer than reacting too slowly during genuine danger.
Ordinarily, higher cortical regions gradually evaluate the situation.
The prefrontal cortex compares current circumstances with previous experience, contextual information, and objective evidence.
If no genuine danger exists, inhibitory signals reduce physiological arousal.
In phobias, this regulatory process becomes less effective.
The alarm system activates with extraordinary intensity, while corrective cognitive mechanisms struggle to reduce the response.
As a result, the body behaves as though survival is immediately threatened.
Heart rate accelerates.
Breathing becomes rapid.
Muscles tense.
Sweating increases.
Attention narrows.
These physiological reactions are entirely real.
Only the source of perceived danger differs from objective reality.
Classical conditioning provides one explanation for phobia development.
A frightening experience occurring in the presence of a neutral object may permanently associate that object with danger.
A child bitten by a dog may later fear all dogs.
A frightening experience during turbulence may contribute to fear of flying.
However, many individuals develop phobias without remembering any traumatic event.
This observation demonstrates that conditioning alone cannot explain every case.
Observational learning also contributes.
Children frequently acquire fears by watching caregivers.
Repeated exposure to anxious parental reactions may teach the developing brain that certain situations deserve fear despite the absence of direct personal danger.
Language further amplifies learning.
Stories, media reports, warnings, and cultural beliefs all influence threat perception.
The brain learns not only through personal experience but also through observation and communication.
Evolutionary psychology offers another intriguing perspective.
Some phobias develop far more easily than others.
Fear of snakes, spiders, heights, darkness, or confined spaces occurs across many cultures.
In contrast, people rarely develop equally intense phobias of electrical outlets, automobiles, or household appliances despite their greater objective danger.
Researchers propose that the human brain evolved biological preparedness for threats commonly encountered throughout evolutionary history.
Ancient dangers continue receiving preferential attention despite dramatic environmental change.
Memory strongly influences phobic reactions.
Emotional memories associated with fear become consolidated efficiently.
Once established, these memories reactivate rapidly whenever similar situations arise.
Importantly, each avoidance behavior prevents the brain from learning that the feared object is actually safe.
Avoidance therefore maintains the disorder.
The individual experiences temporary relief after escaping the feared situation.
This relief reinforces future avoidance.
Over time, fear gradually expands.
A person avoiding one elevator may eventually avoid all elevators.
One uncomfortable experience becomes generalized across increasingly broad situations.
Attention becomes progressively biased toward detecting possible danger.
Individuals with phobias continuously monitor the environment for feared stimuli.
This hypervigilance increases the probability of noticing relevant cues while simultaneously reducing awareness of safety.
The brain therefore receives disproportionate evidence supporting fear.
Neutral experiences receive less attention.
Threat-related information dominates conscious awareness.
Predictive processing models have significantly advanced understanding of phobias.
The brain continuously predicts future events before sensory information arrives.
These predictions influence perception itself.
Individuals with phobias begin anticipating danger long before encountering the feared object.
The body prepares defensively in advance.
Consequently, physiological symptoms often begin before objective exposure occurs.
The individual interprets increased heart rate, dizziness, or muscular tension as evidence confirming danger.
In reality, these bodily sensations result from anticipatory prediction rather than external threat.
Interoception contributes another important mechanism.
The brain constantly interprets signals originating within the body.
Small physiological changes become amplified during anxiety.
Normal increases in heart rate may appear alarming.
Minor dizziness becomes interpreted catastrophically.
This process creates reciprocal interaction.
Fear produces bodily sensations.
Those sensations increase fear.
Greater fear intensifies physiological activation.
The cycle reinforces itself.
Not all phobias involve the same psychological mechanisms.
Specific phobias usually involve clearly identifiable objects or situations.
Social anxiety disorder centers upon fear of negative evaluation by others.
Agoraphobia involves fear of situations in which escape or assistance might be difficult during panic-like symptoms.
Although these disorders share common neurobiological features, each possesses distinctive cognitive patterns requiring individualized clinical understanding.
Genetic influences also contribute significantly.
Family studies demonstrate increased vulnerability among biological relatives.
However, inheritance does not determine specific phobia content.
Genes influence general sensitivity to fear, anxiety regulation, emotional learning, and stress responsiveness.
Environmental experience shapes how these biological predispositions become expressed.
Neuroimaging studies reveal altered communication among the amygdala, hippocampus, insular cortex, anterior cingulate cortex, and prefrontal regions.
Rather than isolated abnormalities, phobias appear to involve dysregulated emotional networks.
The amygdala detects threat rapidly.
The hippocampus contributes contextual memory.
The insula monitors bodily sensations.
Executive regions evaluate evidence and regulate emotional responses.
Successful treatment often strengthens communication among these systems rather than eliminating fear entirely.
Exposure therapy remains one of the most effective psychological interventions.
Contrary to common misunderstanding, exposure therapy does not erase fear memories.
Instead, it creates new learning.
Repeated safe exposure teaches the brain that previously feared situations no longer predict catastrophe.
Original fear memories often remain biologically intact.
New inhibitory memories gradually become stronger.
Recovery therefore reflects learning rather than forgetting.
Pharmacological treatments may reduce symptom intensity in selected individuals, particularly when phobias occur alongside broader anxiety disorders.
However, medication alone rarely changes the underlying learning processes responsible for persistent avoidance.
Behavioral experience remains essential because the nervous system learns safety primarily through direct experience.
One particularly important clinical observation is that insight usually remains preserved.
Most individuals with phobias recognize that their fears are disproportionate.
This distinguishes phobias from psychotic disorders, where beliefs may remain firmly resistant to contradictory evidence.
In phobias, the conflict exists between cognition and emotion.
Logic identifies safety.
The nervous system predicts danger.
These two systems temporarily disagree.
Ultimately, phobias demonstrate that fear is not simply an emotional feeling but a sophisticated biological prediction generated by the brain. The nervous system does not react only to the world as it objectively exists. It reacts to the world as it expects it to be. When prediction systems become excessively sensitive, harmless situations begin activating survival mechanisms designed for genuine emergencies.
Modern psychiatry therefore understands phobias not as failures of courage or willpower but as disorders of emotional learning and threat prediction. The remarkable effectiveness of psychological treatment reflects another equally important truth about the brain: although fear can become deeply learned, the same neuroplastic mechanisms that once created phobias also retain the lifelong capacity to learn safety again.