Among all psychiatric disorders, few are as misunderstood as bipolar disorder, historically referred to as manic-depressive illness. Many people assume that bipolar disorder simply involves alternating periods of happiness and sadness. Modern psychiatry demonstrates that this description is profoundly inaccurate. Mania is not merely an elevated mood, and depression is not simply intense sadness. Both represent complex alterations in brain function involving cognition, emotion, motivation, perception, sleep regulation, reward processing, and self-awareness.
One of the greatest clinical challenges is that bipolar disorder often first appears as depression rather than mania. Many patients seek psychiatric care because of overwhelming hopelessness, fatigue, loss of interest, insomnia, suicidal thoughts, or emotional numbness. During these early episodes, there may be no obvious history of manic symptoms. As a result, bipolar disorder is frequently mistaken for major depressive disorder, sometimes for years before the first clear manic or hypomanic episode emerges.
This delay has important consequences.
Treatment strategies for bipolar depression differ significantly from those used for unipolar depression.
When bipolar disorder remains unrecognized, symptoms may persist, relapse more frequently, or even become destabilized by inappropriate treatment.
Understanding why mania can remain hidden therefore represents one of the most important questions in contemporary mood disorder research.
To appreciate this phenomenon, it is first necessary to understand what psychiatrists mean by mania.
Popular culture often portrays mania as extreme happiness.
In reality, euphoria is only one possible presentation.
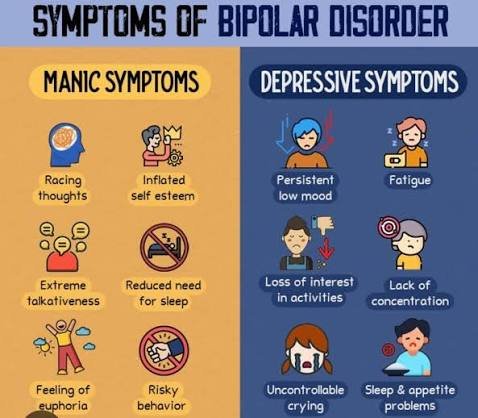
Mania is fundamentally a disorder of mood regulation accompanied by pathological increases in energy, goal-directed behavior, cognitive speed, confidence, and physiological activation.
The individual may sleep only a few hours while feeling fully rested.
Ideas emerge rapidly.
Speech accelerates.
Attention shifts constantly between new possibilities.
Ordinary limitations appear to disappear.
At the same time, judgment frequently deteriorates.
Risk-taking increases.
Financial decisions become impulsive.
Sexual behavior may become unusually uninhibited.
Grandiose beliefs sometimes develop, ranging from exaggerated confidence to psychotic convictions involving extraordinary abilities or special missions.
Importantly, mania is not always pleasant.
Many episodes involve profound irritability rather than euphoria.
The individual becomes impatient, argumentative, emotionally explosive, or intensely suspicious.
Small frustrations provoke disproportionate anger.
The enormous internal energy characteristic of mania may therefore manifest as agitation rather than excitement.
This variability contributes substantially to diagnostic difficulty.
Between severe depression and obvious mania lies hypomania.
Hypomania shares many biological characteristics with mania but occurs at lower intensity.
Individuals remain capable of functioning relatively well.
Some even experience temporary improvements in productivity, creativity, sociability, or confidence.
Because hypomania often feels subjectively positive, many patients do not consider it an illness.
Instead, they describe it as finally feeling “normal” after prolonged depression.
Consequently, clinicians may fail to identify previous hypomanic episodes unless detailed questioning is performed.
This explains why bipolar disorder frequently remains hidden beneath repeated depressive episodes.
Patients naturally focus on experiences that caused suffering.
Periods of increased energy may be forgotten, minimized, or interpreted as healthy recovery.
Family members sometimes recognize behavioral changes more readily than patients themselves.
Mood disorders are increasingly understood through the concept of emotional regulation rather than isolated mood states.
The healthy brain continuously maintains emotional balance despite changing circumstances.
Neural systems regulating reward, motivation, circadian rhythms, stress responses, and executive control remain dynamically coordinated.
Bipolar disorder appears to involve instability within these regulatory systems.
Instead of maintaining equilibrium, mood regulation oscillates between pathological extremes.
Depression and mania therefore represent different expressions of the same underlying dysregulation rather than independent illnesses.
Circadian biology plays an especially important role.
Sleep disturbances often precede manic episodes by days or weeks.
Reduced need for sleep is not simply a symptom of mania.
It may actively contribute to its development.
The brain’s internal biological clock regulates numerous processes, including hormone secretion, body temperature, emotional regulation, cognitive performance, and neurotransmitter activity.
Disruption of circadian rhythms appears capable of destabilizing mood regulation in genetically vulnerable individuals.
This relationship explains why sleep deprivation can sometimes trigger manic episodes.
It also explains why stabilizing sleep often becomes a central component of long-term treatment.
Neurotransmitter systems contribute additional complexity.
Earlier psychiatric models attempted to explain bipolar disorder through simple chemical imbalances involving serotonin, dopamine, or norepinephrine.
Contemporary neuroscience recognizes that the disorder cannot be reduced to abnormalities in a single neurotransmitter.
Instead, large-scale regulatory networks involving multiple neurotransmitter systems appear responsible.
Dopaminergic signaling receives particular attention because dopamine influences reward anticipation, motivation, salience assignment, and goal-directed behavior.
During mania, reward systems appear unusually sensitive.
Ordinary opportunities generate extraordinary motivation.
Novel ideas seem irresistibly important.
The future appears filled with limitless possibility.
Negative consequences receive insufficient attention.
This imbalance contributes significantly to manic decision-making.
One fascinating aspect of bipolar disorder concerns insight.
During severe depression, individuals often recognize that something is profoundly wrong.
During mania, awareness frequently decreases.
The very brain systems responsible for evaluating judgment become altered.
Consequently, patients may reject treatment despite obvious behavioral changes.
From their perspective, they are functioning exceptionally well.
Attempts by family members or clinicians to intervene may appear unnecessary or even threatening.
Psychosis can occur during both manic and depressive episodes.
In manic psychosis, grandiosity frequently dominates.
Individuals may believe they possess extraordinary intelligence, unique spiritual importance, unlimited wealth, or special relationships with powerful figures.
Ideas become increasingly disconnected from objective evidence.
In depressive psychosis, delusions typically revolve around guilt, worthlessness, illness, punishment, or irreversible personal failure.
These contrasting forms illustrate how mood profoundly influences the content of psychotic experience.
Genetic research consistently demonstrates strong hereditary influences.
Among major psychiatric disorders, bipolar disorder possesses one of the highest estimates of genetic contribution.
However, inheritance remains probabilistic rather than deterministic.
No single gene causes bipolar disorder.
Instead, numerous genetic variations interact with developmental experiences, environmental stressors, sleep patterns, substance use, and biological vulnerability.
This complex interaction explains why even identical twins are not always equally affected.
Cognitive functioning also changes across mood episodes.
During mania, thinking often becomes unusually rapid.
Associations form quickly.
Creativity may appear enhanced.
Yet sustained attention deteriorates.
Logical organization weakens.
The individual generates enormous quantities of ideas while evaluating relatively few critically.
This imbalance creates the impression of brilliance despite declining executive control.
Conversely, depression slows cognition dramatically.
Concentration becomes difficult.
Memory feels unreliable.
Decision-making requires tremendous effort.
Even simple tasks appear mentally exhausting.
Importantly, many patients continue experiencing subtle cognitive difficulties even between mood episodes.
These residual impairments may influence occupational functioning and quality of life despite apparent emotional recovery.
One particularly dangerous feature of bipolar disorder involves mixed states.
Contrary to traditional descriptions, depression and mania do not always occur separately.
Some patients simultaneously experience depressive hopelessness alongside manic agitation, racing thoughts, insomnia, irritability, and heightened energy.
These mixed episodes often produce extraordinary psychological distress.
The individual possesses enough energy to act upon suicidal thoughts while remaining overwhelmed by despair.
Modern psychiatry recognizes mixed features as among the highest-risk clinical presentations.
Developmental timing provides another intriguing aspect.
Bipolar disorder commonly emerges during late adolescence or early adulthood, periods characterized by ongoing maturation of neural systems regulating executive control, emotional processing, and reward sensitivity.
Researchers continue investigating why symptoms frequently appear during these developmental transitions rather than earlier in childhood or later adulthood.
Current evidence suggests interactions among brain maturation, hormonal changes, genetic vulnerability, and environmental stress contribute to illness onset.
Longitudinal studies increasingly conceptualize bipolar disorder as a disorder of neural instability rather than isolated episodes.
Even during symptom-free periods, subtle biological differences often remain detectable.
These include alterations in emotional processing, circadian regulation, cognitive flexibility, and neural connectivity.
The illness therefore involves ongoing vulnerability rather than temporary disruption alone.
Treatment reflects this understanding.
Mood stabilizers aim not merely to suppress acute symptoms but to reduce long-term fluctuations.
Psychotherapy helps patients recognize early warning signs, improve emotional regulation, maintain consistent daily routines, and strengthen adherence to treatment.
Sleep stabilization, stress management, and avoidance of psychoactive substances become essential preventive strategies.
Education represents another major therapeutic intervention.
Patients who understand the biological nature of bipolar disorder often recognize mood changes earlier than those who interpret episodes solely through personality or circumstance.
Family education proves equally valuable because relatives frequently notice subtle behavioral changes before patients themselves become aware of them.
Ultimately, the question of whether mania can hide behind depression receives a clear answer from modern psychiatry: it often does. Bipolar disorder may spend years presenting primarily as recurrent depression before hypomania or mania becomes sufficiently obvious for diagnosis. This hidden phase explains why many individuals experience delayed recognition and why careful psychiatric assessment extends far beyond current symptoms alone.
The deeper lesson offered by bipolar disorder concerns the complexity of mood itself. Depression and mania are not simply opposite emotions. They are different expressions of instability within the neural systems responsible for regulating energy, motivation, sleep, cognition, reward, and self-awareness. Understanding this complexity has transformed modern psychiatry, shifting attention away from isolated emotional states toward the dynamic biological networks that continuously maintain the delicate balance underlying human consciousness.