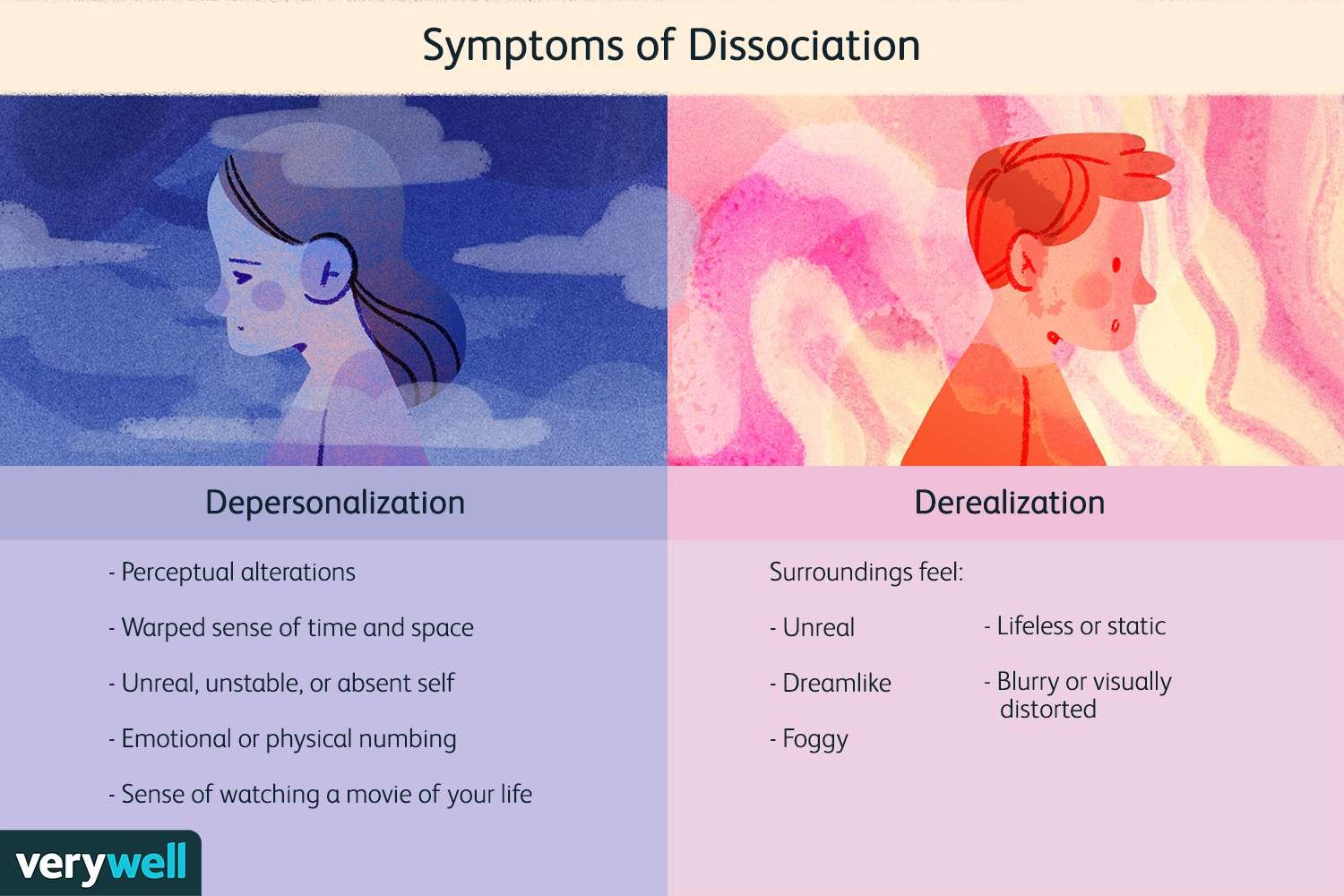
Dissociation is a psychological phenomenon characterized by disruptions in memory, identity, perception, and sense of self. Traditionally associated with trauma and stress, dissociation has also been increasingly linked to sleep disturbances. Recent studies suggest that the boundaries between sleep and wakefulness may play a crucial role in the development and persistence of dissociative symptoms, highlighting a fascinating interplay between neurobiology, consciousness, and psychopathology. Sleep is not a uniform state but a dynamic cycle involving non-rapid eye movement (NREM) and rapid eye movement (REM) phases. These stages are responsible for restoring physical energy, consolidating memory, and regulating emotions. When sleep is disrupted—whether through insomnia, irregular sleep cycles, or parasomnias—boundaries between sleep and wakefulness may blur, creating experiences similar to dissociative states. For example, phenomena such as sleep paralysis, hypnagogic hallucinations, and dream-like intrusions during wakefulness share striking similarities with dissociative symptoms like depersonalization and derealization. Neurobiological evidence supports this connection. Both dissociation and disordered sleep involve dysregulation in the thalamus, prefrontal cortex, and limbic system, regions responsible for sensory integration, emotional regulation, and self-awareness. Abnormalities in REM sleep—where vivid dreaming and emotional processing occur—are particularly associated with dissociative experiences. Inadequate REM regulation may lead to intrusions of dream-like imagery into waking consciousness, contributing to the sense of unreality and detachment characteristic of dissociation. Clinical research also highlights a bidirectional relationship: while sleep disruption can trigger dissociative symptoms, dissociation itself may interfere with healthy sleep patterns. Individuals with post-traumatic stress disorder (PTSD), for example, often experience nightmares, fragmented sleep, and hyperarousal, all of which reinforce dissociative tendencies during the day. Similarly, chronic insomnia has been correlated with higher levels of dissociative experiences in non-clinical populations, suggesting that even in the absence of trauma, sleep instability may foster detachment from reality. From a treatment perspective, addressing sleep disturbances may be a crucial yet underutilized pathway to reducing dissociation. Interventions such as cognitive-behavioral therapy for insomnia (CBT-I), sleep hygiene education, and circadian rhythm stabilization can reduce both sleep-related problems and daytime dissociative symptoms. Pharmacological treatments that regulate sleep architecture, such as certain antidepressants or melatonin, may also provide indirect benefits for dissociation when carefully managed. Furthermore, integrating trauma-focused therapy with sleep-focused interventions can produce synergistic effects in patients with comorbid PTSD and dissociative symptoms. In conclusion, the relationship between sleep and dissociation underscores the importance of viewing consciousness as a continuum rather than a rigid binary between waking and sleeping states. Sleep disruptions can destabilize cognitive and emotional boundaries, giving rise to dissociative phenomena, while dissociation itself may perpetuate sleep problems. Recognizing this interconnection allows clinicians to expand treatment strategies beyond trauma processing alone, incorporating sleep regulation as a key component of recovery. Ultimately, improving sleep may help restore coherence in consciousness, reducing the distressing experiences of fragmentation that define dissociation.

Hidden Rituals in Obsessive-Compulsive Disorder
Obsessive-Compulsive Disorder (OCD) is often portrayed through its most visible features: repetitive handwashing, checking locks, or arranging objects with extreme precision. While these behaviors represent classic compulsions, many individuals with OCD engage in hidden rituals—covert mental acts or subtle behaviors that are far less noticeable but equally distressing. These concealed compulsions contribute to the persistence of the disorder and often complicate both diagnosis and treatment. Hidden rituals can take various forms. Some individuals perform mental compulsions, such as silently repeating prayers, counting numbers, or mentally reviewing past events to neutralize intrusive thoughts. Others may engage in subtle physical behaviors, like tapping objects in a discreet pattern, avoiding certain words in conversation, or blinking in a specific way to “cancel out” unwanted thoughts. Because these behaviors are not outwardly visible, patients may appear unaffected, while in reality they are expending significant mental energy to manage obsessive anxiety. Clinically, hidden rituals are particularly problematic because they blur the line between obsessions and compulsions. Patients may not even recognize these actions as compulsive behaviors, instead perceiving them as natural responses to unwanted thoughts. This lack of awareness can delay diagnosis and reduce treatment effectiveness. Moreover, because hidden rituals do not attract external attention, family members, teachers, or even clinicians may underestimate the severity of the disorder. Neurobiologically, hidden rituals are thought to arise from the same dysfunctions implicated in classical OCD: abnormalities in cortico-striato-thalamo-cortical (CSTC) circuits, heightened error detection in the anterior cingulate cortex, and altered serotonin and dopamine regulation. These mechanisms create a powerful drive to reduce perceived threats or internal discomfort, even when the behavior providing relief is purely mental. From a therapeutic perspective, hidden rituals present unique challenges. Standard exposure and response prevention (ERP), a core component of cognitive-behavioral therapy, relies on preventing compulsive responses to anxiety-inducing stimuli. However, when compulsions are covert, it is more difficult for clinicians to monitor whether patients are resisting their rituals. Specialized strategies, such as “imaginal exposure,” self-monitoring logs, and therapist-guided awareness training, are often necessary to address these invisible behaviors. Pharmacological treatments, particularly SSRIs and clomipramine, remain important tools, but they are most effective when combined with psychotherapeutic approaches that directly target covert compulsions. In conclusion, hidden rituals represent an underrecognized but critical dimension of OCD. Though less visible than handwashing or checking, these mental and subtle behavioral compulsions can be equally debilitating, consuming time, energy, and emotional resources. Greater awareness of hidden rituals is essential for accurate diagnosis, effective therapy, and improved outcomes. By bringing these invisible struggles into focus, clinicians can ensure that the full spectrum of OCD symptoms is addressed, offering patients a more comprehensive path to recovery.
The Paradoxical Effects of Antidepressants: When Treatment Challenges Expectations
Antidepressants are among the most widely prescribed psychiatric medications, primarily used for major depressive disorder, anxiety disorders, and related conditions. While their therapeutic goal is to alleviate symptoms and restore emotional balance, a paradox has emerged in clinical practice: in certain cases, antidepressants can produce unexpected and counterintuitive effects. These paradoxical reactions include worsening of depressive symptoms, emergence of suicidal thoughts, induction of mania in bipolar disorder, or emotional blunting. Understanding these outcomes is critical for both clinicians and patients, as they complicate treatment and highlight the complexity of brain chemistry. One of the most widely discussed paradoxical effects is the early increase in suicidal ideation, particularly in adolescents and young adults treated with selective serotonin reuptake inhibitors (SSRIs). Although the mechanism is not fully understood, it is hypothesized that SSRIs may initially improve psychomotor energy before mood elevation occurs, creating a dangerous window in which individuals have more energy to act on suicidal impulses. This phenomenon has led to black box warnings and increased monitoring recommendations in younger populations. Another paradoxical reaction is the switching phenomenon observed in individuals with bipolar disorder. Antidepressants, especially when prescribed without a mood stabilizer, can precipitate manic or hypomanic episodes. This effect underscores the importance of accurate diagnosis, as bipolar disorder may initially present with depressive symptoms alone, leading to misdiagnosis as unipolar depression. In such cases, antidepressant treatment can destabilize mood rather than stabilize it, complicating long-term management. A subtler but clinically significant paradox is emotional blunting or flattening, in which patients report feeling emotionally numb, detached, or indifferent. While these symptoms may represent partial relief from intense negative affect, they can also reduce positive emotional experiences, impairing quality of life. Neurobiological explanations point to alterations in serotonin and dopamine pathways that regulate both negative and positive affect. Additionally, paradoxical anxiety or agitation may occur when initiating antidepressants, particularly SSRIs or SNRIs. Some patients experience heightened restlessness, insomnia, or irritability during the first weeks of treatment. This side effect, often temporary, highlights the delicate balance of neurotransmitter systems and underscores the importance of gradual titration and patient education. From a clinical standpoint, paradoxical effects raise important questions about personalized psychiatry. Genetic variability in drug metabolism (pharmacogenomics), differences in receptor sensitivity, and unique psychosocial contexts all influence whether a patient experiences benefit or paradoxical harm. Increasingly, clinicians are exploring individualized treatment strategies, including pharmacogenetic testing, close monitoring in early treatment phases, and combined pharmacological-psychotherapeutic approaches. In conclusion, while antidepressants remain indispensable tools in modern psychiatry, their paradoxical effects challenge the assumption that pharmacological treatment is universally stabilizing. Recognizing, anticipating, and monitoring these counterintuitive reactions is essential for patient safety and treatment success. Future advances in precision psychiatry may reduce the risk of paradoxical responses by tailoring interventions to individual biological and psychological profiles, ultimately transforming the way antidepressants are prescribed and managed.
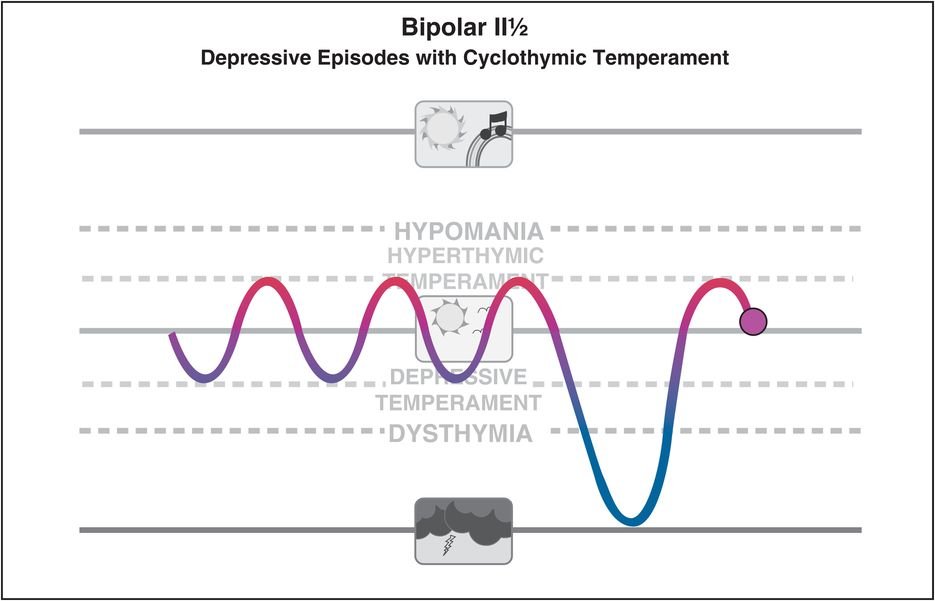
Micro Mood Fluctuations in Bipolar Disorder: Beyond Classic Episodes
Bipolar disorder is traditionally characterized by distinct episodes of mania, hypomania, and depression. These well-defined phases form the cornerstone of diagnosis and treatment. However, emerging research highlights a subtler phenomenon: micro mood fluctuations. Unlike the pronounced shifts observed in classic episodes, micro fluctuations involve rapid, often hour-to-hour or day-to-day changes in mood, energy, and activity levels. These subtle variations are frequently overlooked in clinical settings but can significantly affect the daily functioning and quality of life of individuals with bipolar disorder. Micro mood fluctuations can manifest as brief periods of irritability, mild elation, or transient low mood that do not meet full criteria for manic or depressive episodes. Despite their small scale, these fluctuations may disrupt attention, social interactions, and decision-making. In some cases, patients with prominent micro fluctuations are misdiagnosed with personality disorders or anxiety disorders because their mood patterns do not fit the classical bipolar framework. The neurobiological mechanisms underlying micro mood fluctuations are not yet fully understood. Dysregulation in circadian rhythms, neurotransmitter imbalances (particularly in dopamine and serotonin systems), and heightened neural sensitivity to stressors have all been implicated. Functional neuroimaging studies suggest that abnormal connectivity between the prefrontal cortex and limbic system may contribute to rapid shifts in emotional regulation. Additionally, environmental triggers such as sleep disruption, psychosocial stress, or substance use can exacerbate these subtle mood swings. Recognition of micro mood fluctuations has important clinical implications. Standard mood charts and traditional diagnostic interviews may fail to capture these brief but impactful episodes. Increasingly, clinicians are employing daily mood monitoring, digital apps, and ecological momentary assessment (EMA) to track these fluctuations more accurately. This data allows for more personalized treatment approaches, including adjustments in medication, psychotherapy strategies, and lifestyle interventions aimed at stabilizing daily mood patterns. Therapeutically, micro mood fluctuations challenge conventional pharmacotherapy. While lithium, anticonvulsants, and atypical antipsychotics are effective in controlling full-blown manic or depressive episodes, their impact on subthreshold mood instability is less robust. Adjunctive interventions such as structured routines, cognitive-behavioral therapy, and psychoeducation for patients and families can improve self-awareness and coping strategies. Targeting sleep hygiene, stress reduction, and regular activity schedules also plays a critical role in mitigating micro fluctuations. In conclusion, micro mood fluctuations represent a nuanced and clinically significant feature of bipolar disorder that extends beyond classic episodes. These subtle shifts in affect can impair daily functioning, complicate diagnosis, and challenge treatment. Greater awareness and systematic monitoring of micro fluctuations are essential for comprehensive care. Integrating pharmacological, behavioral, and lifestyle interventions tailored to these fluctuations may enhance quality of life and reduce the long-term burden of bipolar disorder.
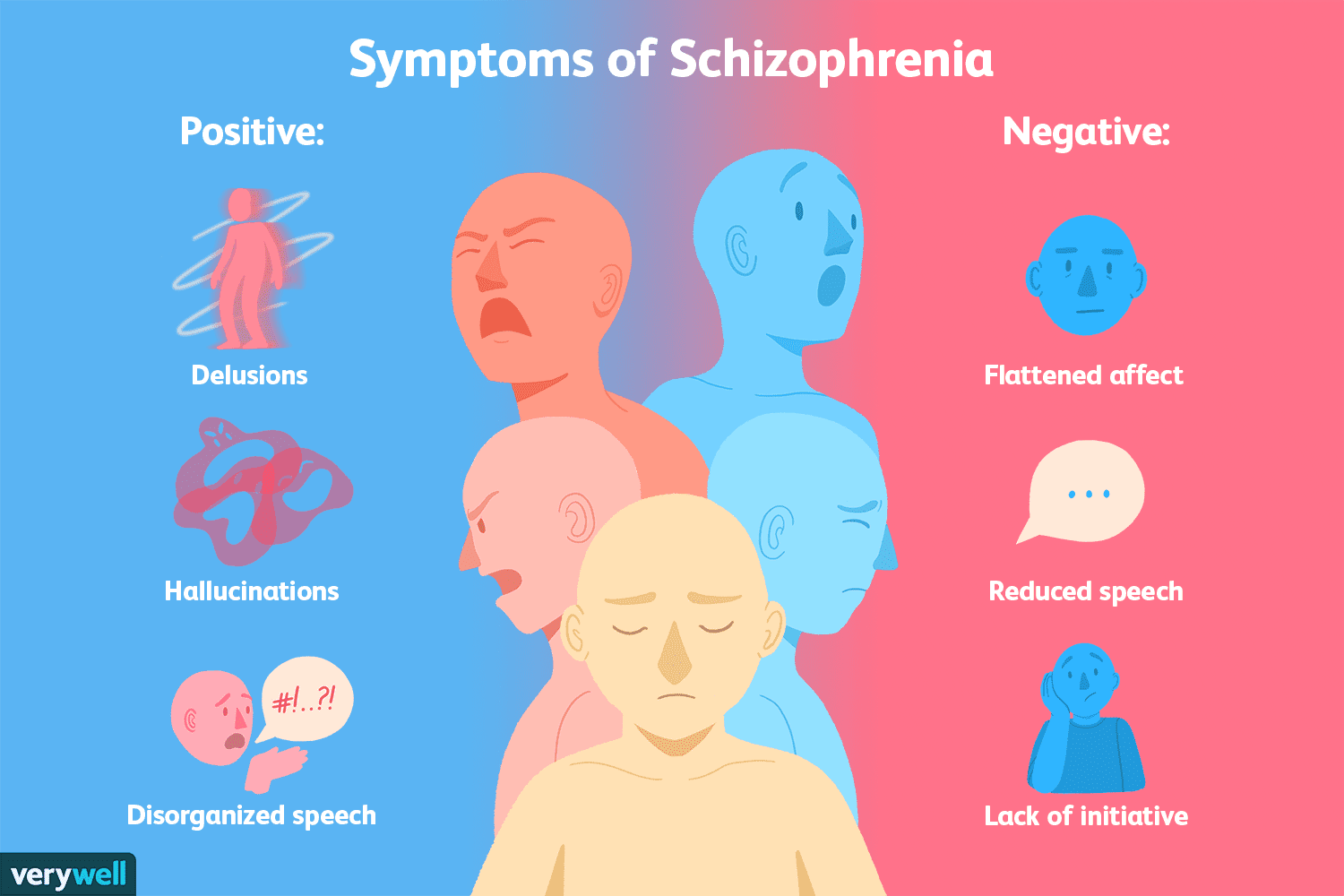
Negative Symptoms in Schizophrenia: The Silent Struggle
Schizophrenia is often recognized by its most conspicuous features: hallucinations, delusions, and disorganized speech or behavior. These positive symptoms dominate clinical and public perception of the disorder. However, there exists a set of negative symptoms—subtle, persistent, and often overlooked—that can be far more disabling in daily life. Negative symptoms include emotional blunting, reduced motivation (avolition), diminished speech output (alogia), social withdrawal, and anhedonia (the inability to experience pleasure). Despite their clinical significance, these symptoms are frequently underrepresented in research and popular discourse, earning them the label of the “silent symptoms” of schizophrenia. Negative symptoms are particularly challenging because they are less responsive to traditional antipsychotic medications, which primarily target positive symptoms through dopaminergic modulation. As a result, patients may experience persistent functional impairment despite adequate control of hallucinations or delusions. Emotional blunting, for instance, reduces the capacity for normal affective expression, making interpersonal interactions difficult. Social withdrawal and avolition can prevent patients from engaging in work, education, or social activities, significantly decreasing quality of life. Recent research suggests that negative symptoms may stem from complex neurobiological mechanisms, including dysregulation in the prefrontal cortex, hypoactivity in mesocortical dopamine pathways, and alterations in glutamatergic neurotransmission. These deficits impact cognitive and executive functions, compounding the challenges imposed by social and emotional withdrawal. Furthermore, environmental factors, such as early life stress or social isolation, may exacerbate negative symptoms by influencing brain development and neural connectivity. One of the key challenges in diagnosing and treating negative symptoms is their subtlety. Unlike hallucinations or delusions, which are observable and easily reported, negative symptoms may be mistaken for depression, medication side effects, or lack of engagement. Clinicians must therefore carefully distinguish between these conditions through structured assessments and longitudinal observation. Tools such as the Scale for the Assessment of Negative Symptoms (SANS) or the Positive and Negative Syndrome Scale (PANSS) can aid in this evaluation, providing standardized measures of symptom severity. Innovative therapeutic approaches are emerging to address these silent symptoms. Psychosocial interventions, including cognitive behavioral therapy, social skills training, and vocational rehabilitation, have shown promise in enhancing functional outcomes. Additionally, newer pharmacological strategies targeting glutamatergic and cholinergic systems are being investigated, aiming to directly improve negative symptomatology. Research into the role of inflammation and immune dysregulation also suggests potential novel avenues for intervention. In conclusion, negative symptoms in schizophrenia represent a critical yet frequently overlooked dimension of the disorder. They profoundly affect patients’ daily functioning and quality of life, often persisting even when positive symptoms are controlled. Greater awareness, early detection, and comprehensive treatment strategies that integrate pharmacological and psychosocial approaches are essential to addressing the silent struggles of individuals living with schizophrenia. Recognizing and targeting these symptoms is not only crucial for clinical management but also for improving long-term social, occupational, and emotional outcomes.

Microbiota and the Brain: New Horizons in Psychiatry
For many years, psychiatry primarily explained disorders such as depression, anxiety, and schizophrenia through imbalances in brain chemicals. However, recent research has revealed that the trillions of microorganisms residing in our digestive system—known as the gut microbiota—may have a far more profound impact on mental health than previously thought. These microorganisms do more than regulate digestion; they influence the production of neurotransmitters such as serotonin, dopamine, and GABA, which directly affect brain function. Remarkably, approximately 90% of the body’s serotonin is produced in the gut. Communication between the gut and the brain occurs through several pathways. Via the vagus nerve, signals from the gut are transmitted directly to the brain. Animal studies have shown that certain bacteria reduce anxiety only when the vagus nerve is intact. Chemically, the microbiota influences neurotransmitter production, while the immune system pathway allows imbalances in the gut—known as dysbiosis—to trigger chronic inflammation, which is linked to psychiatric disorders such as depression and schizophrenia. This demonstrates how even minor disturbances in the gut can significantly affect brain function. The relationship between the microbiota and psychiatric disorders is increasingly recognized. In depression, studies have found reduced diversity in the gut flora compared to healthy individuals, and probiotic supplementation has sometimes alleviated depressive symptoms. In anxiety disorders, species such as Lactobacillus and Bifidobacterium have shown anxiolytic effects. In schizophrenia, gut bacteria appear to influence dopamine metabolism, potentially affecting the course of the disorder. In autism spectrum disorder, alterations in gut microbiota have been observed, and certain probiotic interventions have shown improvements in social behaviors and repetitive actions. The emerging concept of “psychobiotics” refers to probiotics that have a positive effect on mental health. For example, Lactobacillus rhamnosus has been shown in animal studies to reduce anxiety, while Bifidobacterium longum can alleviate depressive symptoms. These findings suggest that psychobiotics may, in the future, serve as complementary or alternative treatments to conventional antidepressants. In daily life, supporting the gut-brain axis involves consuming a diet rich in fiber, minimizing processed and additive-laden foods, maintaining regular sleep, and engaging in physical activity. These practices not only support gut health but also positively influence mental well-being. The gut microbiota is not merely a system for digestion; it is a powerful biological mechanism that influences brain function and mood. Disorders such as depression, anxiety, schizophrenia, and autism may involve both chemical imbalances in the brain and disruptions in gut health. In the future, psychiatry is expected to increasingly incorporate multi-dimensional treatment approaches that combine medication, nutrition, probiotic supplementation, and inflammation management.

Sleep and Memory: The Hidden Role of Micro-Arousals
Sleep is widely known as essential for memory and learning, yet the subtle mechanisms of how the brain processes experiences during the night are still being uncovered. One of the most intriguing discoveries in recent sleep research is the role of micro-arousals—very brief moments when the brain partially “wakes up” without the sleeper being aware. Far from being disruptive, these micro-arousals may actually play a critical role in consolidating memories and regulating emotions. During normal sleep, the brain cycles through different stages, including light sleep, deep sleep, and REM (rapid eye movement) sleep. Traditionally, uninterrupted cycles were considered ideal. However, advanced neuroimaging and EEG studies have shown that micro-arousals—lasting just a few seconds—occur naturally throughout the night. In fact, healthy adults experience dozens, sometimes even hundreds, of them without realizing it. These short awakenings serve as neural checkpoints. They allow the brain to briefly assess the body’s safety and adjust sleep depth accordingly. But beyond this protective function, they appear to act as windows for memory processing. Research from European sleep laboratories suggests that micro-arousals create opportunities for the hippocampus—the brain’s memory hub—to transfer information to the neocortex, where long-term memories are stored. Without these micro-awakenings, certain memories might remain fragmented or fail to integrate fully into long-term storage. Interestingly, the quality of micro-arousals matters. When they occur naturally, they are part of healthy sleep architecture. But when caused by external disturbances—like loud noises, sleep apnea, or excessive stress—they can fragment sleep and impair memory instead of strengthening it. This highlights the delicate balance between necessary micro-arousals and disruptive awakenings. Another hidden benefit of micro-arousals is emotional recalibration. Sleep is not only about storing facts but also about processing feelings. These short neural resets may give the brain brief opportunities to regulate emotional intensity, ensuring that painful or stressful memories are softened by morning. This could explain why people often feel less emotionally overwhelmed about events after a night’s sleep. From a practical perspective, this knowledge challenges the common belief that only completely “deep, uninterrupted” sleep is valuable. Instead, healthy sleep includes tiny fluctuations—moments of near-wakefulness—that quietly support memory, creativity, and emotional health. Protecting sleep from excessive disturbances while allowing natural micro-arousals may be one of the keys to unlocking the brain’s full restorative power.

The Hidden Emotional Effects of Digital Minimalism
In today’s hyperconnected world, digital devices dominate nearly every aspect of daily life. Smartphones, social media, and constant notifications offer convenience, but they also create invisible psychological costs. While the obvious impacts of excessive screen time—reduced attention span, sleep disruption, and stress—are widely discussed, neuroscience and psychology reveal several hidden effects of digital minimalism that are far less known but deeply valuable. One surprising insight is the role of eye contact and trust. When partners or friends spend less time on their devices, their face-to-face interactions naturally increase. Neuroscience shows that direct eye contact triggers the release of oxytocin, often called the “bonding hormone,” which strengthens feelings of safety and connection. By contrast, the simple act of glancing at a phone during conversation—sometimes called “phubbing”—can unconsciously reduce perceived empathy and trust, even if the person insists they are listening. Another overlooked effect is the restoration of the brain’s default mode network (DMN). This network becomes active during moments of quiet reflection or daydreaming and is essential for creativity, memory consolidation, and self-identity. Constant digital stimulation disrupts DMN activity, leaving the brain overstimulated but under-reflective. Digital minimalism, even in small doses such as phone-free mornings, allows the DMN to reactivate, leading to richer ideas and stronger self-awareness. Digital minimalism also influences dopamine regulation. Social media platforms are designed around unpredictable rewards—likes, messages, or viral content—which hijack the brain’s reward system in the same way gambling does. By reducing digital exposure, individuals give their dopamine circuits time to reset, leading to greater sensitivity to natural rewards such as real conversations, physical activity, or nature. This “dopamine recalibration” enhances long-term motivation and emotional stability. Finally, minimalism in the digital realm creates psychological spaciousness. When people reduce screen use, they often notice an unexpected emotional shift: feelings of calm, patience, and present-moment awareness grow stronger. This happens because the constant cognitive load of switching between apps, notifications, and tasks is lifted, freeing mental energy for deeper engagement with life. In short, digital minimalism is not simply about spending less time on a phone. It is about restoring trust in relationships, reactivating creative brain networks, resetting reward systems, and rediscovering calm. By intentionally designing a digital environment that supports rather than controls us, we gain more than productivity—we gain emotional clarity and stronger human connection.

How the Brain Reacts to Uncertainty
Uncertainty is one of the most stressful conditions for the human brain. From deciding whether a job opportunity will succeed to waiting for medical results, situations filled with unpredictability often cause anxiety. Neuroscience shows that our brains are wired to dislike uncertainty because it interferes with the primary function of the nervous system: predicting and preparing for the future. Yet beyond this surface reaction, the brain’s response to uncertainty reveals surprising and lesser-known insights. The amygdala, the brain’s threat detection center, is highly sensitive to unpredictable situations. When the brain cannot predict outcomes, the amygdala activates stress pathways, releasing cortisol and increasing vigilance. Interestingly, studies have found that the brain often perceives uncertainty as more stressful than guaranteed negative outcomes. For example, people may feel calmer knowing they will experience a painful shock than waiting to find out whether a shock will happen at all. This highlights how much the brain prioritizes certainty—even when the certainty is unpleasant. But uncertainty is not only a source of stress; it also engages the prefrontal cortex, the area responsible for flexible thinking and problem-solving. When predictable routines break down, the brain is forced to explore new possibilities. This is why uncertainty can also fuel creativity and innovation. Historical evidence shows that crises—whether economic, social, or personal—often lead to major breakthroughs, precisely because the brain is pushed out of its habitual comfort zone. Another hidden aspect is how uncertainty interacts with the brain’s reward system. Dopamine, often called the “motivation molecule,” is not only released when we receive rewards but also when rewards are unpredictable. This is why gambling or checking social media notifications can be so addictive—the uncertainty itself becomes stimulating. The brain essentially finds excitement in not knowing what comes next, creating a paradox where uncertainty is both stressful and rewarding. On a deeper level, neuroscience reveals that individual tolerance for uncertainty varies. People with higher activity in the anterior cingulate cortex, a region that monitors errors and conflicts, are better at adapting to unpredictability. This means resilience in uncertain times is not just psychological—it has measurable neural foundations. Moreover, training practices such as mindfulness have been shown to quiet the amygdala while strengthening prefrontal regulation, effectively rewiring the brain to handle uncertainty with greater calm. In conclusion, the brain’s reaction to uncertainty is complex and multifaceted. While it naturally triggers fear and stress through the amygdala, it also stimulates creativity, adaptability, and even excitement through the prefrontal cortex and dopamine pathways. Uncertainty is not only a threat but also a hidden opportunity for growth, depending on how the brain learns to process it. By understanding these mechanisms, we can shift from resisting uncertainty to using it as a catalyst for resilience and innovation.

Hidden Dimensions of Couples Therapy: Insights Beyond Common Knowledge
When most people think of couples therapy, the first concepts that come to mind are communication, trust, and conflict resolution. While these are undeniably important, therapy in practice often addresses much deeper and less obvious dimensions of relationships—dimensions that are rarely discussed in mainstream articles but play a crucial role in healing and growth. One lesser-known aspect of couples therapy is the exploration of attachment styles. Research shows that the way individuals bonded with their caregivers in childhood influences how they connect with partners in adulthood. For example, someone with an anxious attachment style may constantly seek reassurance, while a partner with avoidant tendencies may withdraw under stress. In therapy, uncovering these hidden patterns helps couples understand that recurring conflicts are not simply about “bad behavior” but about deeply rooted emotional strategies for seeking safety. This awareness alone often reduces blame and increases compassion. Another dimension is the role of unspoken expectations. Every person enters a relationship with invisible “rules” shaped by culture, family history, or personal values. These rules may involve how affection should be expressed, who manages finances, or how conflicts should be handled. Problems arise when these expectations remain unvoiced. In therapy, bringing them to light allows partners to renegotiate their “relationship contract” in a way that feels fair and conscious rather than automatic and inherited. Couples therapy also examines the impact of micro-interactions. Studies show that it is not just major conflicts but small, daily exchanges that shape the health of a relationship. Eye contact, tone of voice, brief gestures of appreciation—or their absence—accumulate over time. Therapists often train couples to notice and change these micro-moments, because strengthening them can be more transformative than resolving a single large argument. An underexplored yet powerful tool in therapy is repair attempts. Research by Dr. John Gottman highlights that the success of a relationship is not about avoiding conflict, but about how effectively partners make and respond to repair attempts—those small signals like humor, a gentle touch, or a simple “I didn’t mean that” during or after a disagreement. Couples who recognize and accept these bids for repair tend to thrive, while those who miss them often spiral into resentment. Finally, therapy addresses the intergenerational influence. Unresolved patterns from family history—such as divorce, financial struggles, or unhealthy coping strategies—often echo into present relationships. Couples therapy creates space to identify and break these cycles, ensuring that old wounds do not dictate the future of the partnership. In essence, couples therapy is not just about learning to “communicate better.” It is about uncovering hidden layers—attachment patterns, invisible expectations, micro-interactions, repair strategies, and family legacies—that shape how partners connect. By bringing these deeper insights into awareness, couples not only resolve conflicts but also create a more conscious, resilient, and authentic bond.