Among the most fascinating questions in modern psychiatry is why the human brain sometimes becomes unable to release a single thought. Every healthy mind produces countless unwanted ideas throughout the day. Violent images, inappropriate words, irrational fears, embarrassing memories, and bizarre possibilities briefly enter consciousness before disappearing almost immediately. Most people hardly notice them. Yet in obsessive-compulsive disorder (OCD), these same ordinary mental events become persistent, emotionally overwhelming, and nearly impossible to ignore. The central mystery is not why intrusive thoughts exist—they occur in nearly everyone—but why certain brains assign extraordinary importance to thoughts that would otherwise be dismissed.
For decades, obsessive thoughts were misunderstood as evidence of unusual personality traits or hidden unconscious desires. Contemporary psychiatry has largely abandoned these explanations. Research increasingly demonstrates that obsessions arise from abnormalities in cognitive control, uncertainty processing, threat detection, emotional regulation, and neural circuits responsible for evaluating significance. The problem is not that individuals with OCD think differently from everyone else. The problem is that their brains respond differently to the same kinds of thoughts experienced by the general population.
The first principle in understanding obsessions is recognizing that the brain continuously filters information.
Every second, countless thoughts, sensations, memories, and perceptions compete for conscious attention.
Most are automatically discarded.
This filtering system allows attention to remain focused on information that is genuinely important.
Without it, consciousness would become overwhelmed by irrelevant mental activity.
In OCD, this filtering process appears to malfunction.
Instead of allowing intrusive thoughts to pass naturally, the brain repeatedly identifies them as highly significant.
A random thought such as “Did I lock the door?” no longer remains an ordinary question.
It becomes an unresolved threat.
The mind begins treating uncertainty itself as danger.
Modern neuroscience suggests that this process involves abnormal activity within cortico-striato-thalamo-cortical circuits. These interconnected brain networks help regulate decision-making, error detection, habit formation, and behavioral inhibition. Rather than switching attention away from completed concerns, these circuits continue signaling that something remains unresolved.
The result is a persistent internal message that the task is incomplete.
Even when objective evidence clearly indicates safety, the brain continues generating doubt.
This persistent doubt represents one of OCD’s defining characteristics.
Patients rarely seek absolute certainty because they enjoy certainty.
They seek it because their nervous system struggles to tolerate uncertainty itself.
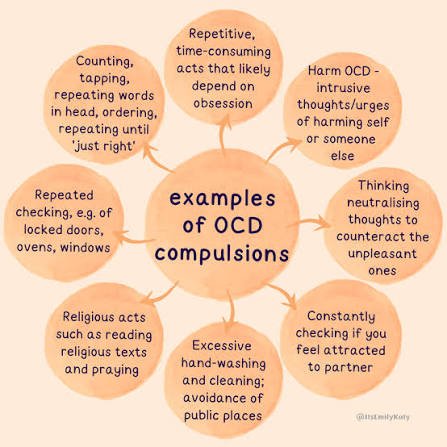
The emotional experience becomes so uncomfortable that repeated checking, washing, counting, or reassurance temporarily reduces distress.
Unfortunately, this relief is short-lived.
Each ritual teaches the brain that the obsession deserved attention.
Consequently, future intrusive thoughts become even more convincing.
A self-reinforcing cycle develops.
Compulsions therefore do not merely accompany obsessions.
They strengthen them.
Another remarkable feature of OCD is thought-action fusion.
Many patients gradually begin experiencing thoughts as morally or physically equivalent to actions.
An intrusive image of harming someone may feel almost as disturbing as actually committing violence.
The individual recognizes intellectually that no action has occurred.
Emotionally, however, guilt and responsibility remain overwhelming.
This explains why people with OCD are often among the least likely individuals to act upon their intrusive thoughts.
The thoughts themselves are profoundly inconsistent with their values.
Precisely because they care deeply about preventing harm, the brain becomes trapped monitoring every possible threat.
Neuroimaging studies reveal that regions involved in error monitoring frequently show increased activity in OCD.
The brain behaves as though mistakes are constantly about to occur.
Even ordinary uncertainty activates systems normally reserved for genuine danger.
This exaggerated error signal influences virtually every aspect of cognition.
Simple decisions become exhausting.
Completed tasks continue feeling unfinished.
Reassurance loses effectiveness because the internal warning system remains active.
The person is not searching for information.
They are searching for a feeling of certainty that never fully arrives.
Memory is also affected.
Contrary to popular assumptions, many individuals with OCD possess intact or even excellent memory.
The difficulty lies not in remembering but in trusting memory.
Repeated checking gradually weakens confidence.
After verifying a locked door multiple times, individual checking episodes become difficult to distinguish.
Memory becomes less vivid precisely because the behavior has been repeated excessively.
The resulting uncertainty encourages further checking.
Again, the disorder maintains itself through recursive learning.
One of the most important developments in contemporary psychiatry involves predictive processing models.
The brain continuously predicts what should happen next and updates these predictions according to incoming evidence.
In OCD, prediction systems appear unusually sensitive to low-probability negative outcomes.
Tiny possibilities receive disproportionate attention.
Although the individual recognizes that catastrophe is unlikely, the nervous system behaves as though unlikely events require immediate prevention.
This explains why logical reassurance often provides limited benefit.
The difficulty lies within predictive learning rather than factual knowledge.
Emotion plays a central role throughout this process.
Obsessions persist not because they contain important information but because they acquire intense emotional salience.
Fear, guilt, disgust, responsibility, and uncertainty combine to create unusually powerful learning signals.
The brain mistakenly concludes that emotionally intense thoughts must also be objectively important.
In reality, emotional intensity and factual significance are not equivalent.
Developmental experiences may influence vulnerability as well.
Genetic factors contribute substantially to OCD risk, yet environmental learning shapes symptom content.
Children raised in highly unpredictable or excessively responsibility-focused environments may become particularly sensitive to uncertainty.
However, OCD cannot be explained solely through upbringing.
Twin studies consistently demonstrate significant biological contributions involving multiple genes interacting with developmental experiences.
One particularly fascinating observation is that obsessional themes vary across cultures while underlying mechanisms remain remarkably similar.
Some individuals fear contamination.
Others fear blasphemy.
Others become preoccupied with symmetry, morality, illness, sexuality, relationships, or memory.
Despite these differences, the underlying psychological architecture remains consistent.
An intrusive thought becomes assigned excessive significance.
Uncertainty becomes intolerable.
Compulsive behavior temporarily reduces distress.
Negative reinforcement strengthens the cycle.
Modern treatment reflects this understanding.
Exposure and response prevention therapy gradually teaches the brain that uncertainty can be tolerated without performing compulsions.
Rather than proving feared outcomes impossible, therapy reduces the perceived necessity of achieving perfect certainty.
Over time, neural learning begins changing.
The internal alarm system gradually becomes less reactive.
Medications influencing serotonin transmission often complement psychotherapy by reducing symptom intensity, although their precise mechanisms remain more complex than simple neurotransmitter correction.
Perhaps the deepest lesson offered by OCD concerns the nature of human thought itself.
Healthy psychological functioning depends not upon controlling every thought but upon allowing most thoughts to pass without assigning them excessive meaning.
The mind continuously generates possibilities, many of which are irrelevant or irrational.
Mental health depends partly upon recognizing that a thought is not a prediction, not an intention, not a memory, and not a moral statement.
It is often simply a transient product of normal brain activity.
In obsessive-compulsive disorder, this distinction becomes blurred.
The brain begins treating possibilities as probabilities and uncertainty as immediate danger.
Ultimately, obsessive thoughts reveal something fundamental about consciousness. The brain is not merely a machine that produces thoughts; it is a machine that decides which thoughts deserve attention. OCD emerges when this system of assigning significance becomes dysregulated. The disorder does not arise because the mind generates uniquely strange ideas. It arises because ordinary intrusive thoughts become trapped within neural circuits that refuse to classify them as unimportant.
In this sense, obsessions are not failures of intelligence or willpower. They are the consequence of highly sophisticated brain systems becoming excessively devoted to preventing uncertainty, error, and harm. The tragic irony is that the very mechanisms designed to protect human beings from danger gradually become the source of persistent psychological suffering.