Dissociation is a psychological phenomenon characterized by disruptions in memory, identity, perception, and sense of self. Traditionally associated with trauma and stress, dissociation has also been increasingly linked to sleep disturbances. Recent studies suggest that the boundaries between sleep and wakefulness may play a crucial role in the development and persistence of dissociative symptoms, highlighting a fascinating interplay between neurobiology, consciousness, and psychopathology.
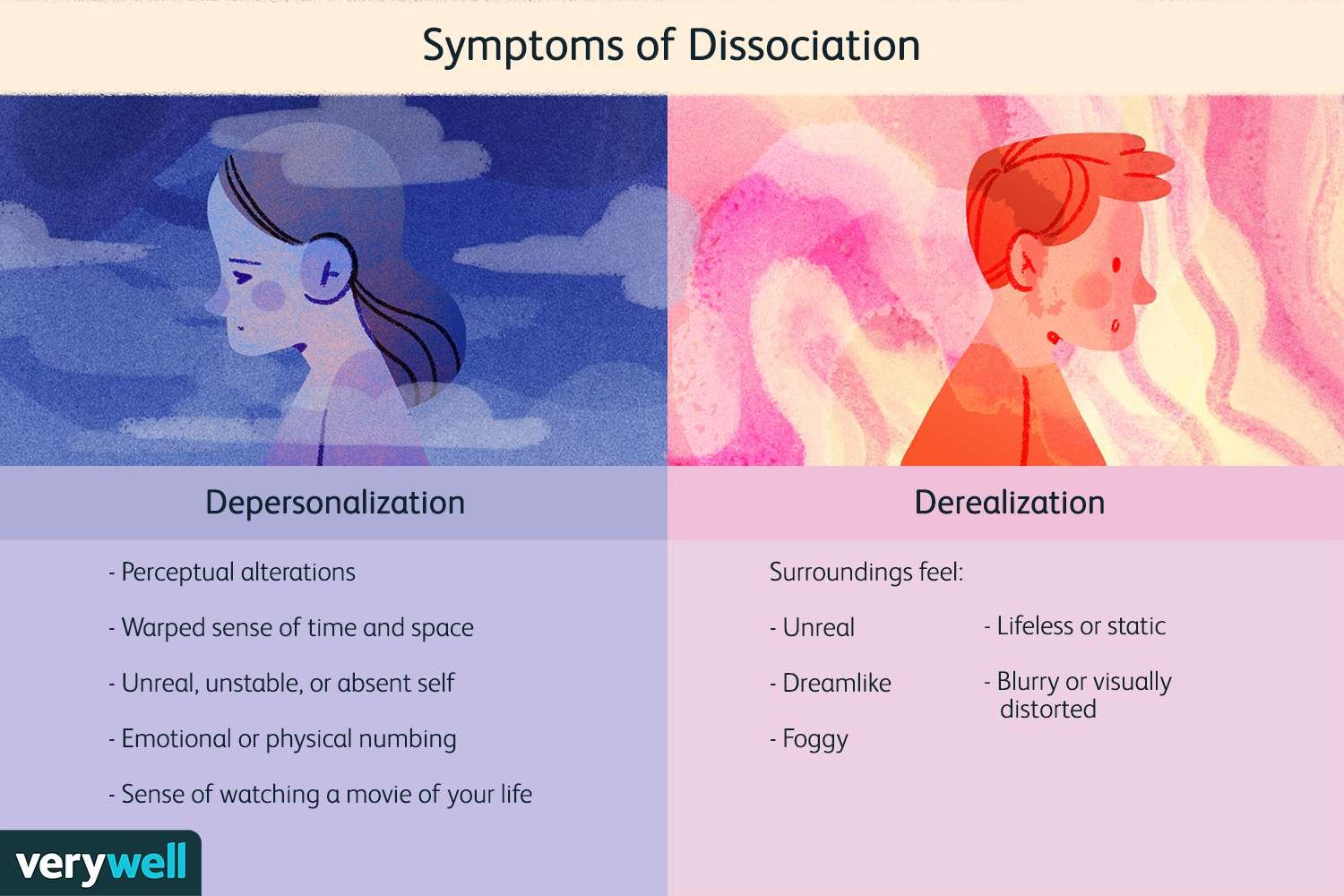
Sleep is not a uniform state but a dynamic cycle involving non-rapid eye movement (NREM) and rapid eye movement (REM) phases. These stages are responsible for restoring physical energy, consolidating memory, and regulating emotions. When sleep is disrupted—whether through insomnia, irregular sleep cycles, or parasomnias—boundaries between sleep and wakefulness may blur, creating experiences similar to dissociative states. For example, phenomena such as sleep paralysis, hypnagogic hallucinations, and dream-like intrusions during wakefulness share striking similarities with dissociative symptoms like depersonalization and derealization.
Neurobiological evidence supports this connection. Both dissociation and disordered sleep involve dysregulation in the thalamus, prefrontal cortex, and limbic system, regions responsible for sensory integration, emotional regulation, and self-awareness. Abnormalities in REM sleep—where vivid dreaming and emotional processing occur—are particularly associated with dissociative experiences. Inadequate REM regulation may lead to intrusions of dream-like imagery into waking consciousness, contributing to the sense of unreality and detachment characteristic of dissociation.
Clinical research also highlights a bidirectional relationship: while sleep disruption can trigger dissociative symptoms, dissociation itself may interfere with healthy sleep patterns. Individuals with post-traumatic stress disorder (PTSD), for example, often experience nightmares, fragmented sleep, and hyperarousal, all of which reinforce dissociative tendencies during the day. Similarly, chronic insomnia has been correlated with higher levels of dissociative experiences in non-clinical populations, suggesting that even in the absence of trauma, sleep instability may foster detachment from reality.
From a treatment perspective, addressing sleep disturbances may be a crucial yet underutilized pathway to reducing dissociation. Interventions such as cognitive-behavioral therapy for insomnia (CBT-I), sleep hygiene education, and circadian rhythm stabilization can reduce both sleep-related problems and daytime dissociative symptoms. Pharmacological treatments that regulate sleep architecture, such as certain antidepressants or melatonin, may also provide indirect benefits for dissociation when carefully managed. Furthermore, integrating trauma-focused therapy with sleep-focused interventions can produce synergistic effects in patients with comorbid PTSD and dissociative symptoms.
In conclusion, the relationship between sleep and dissociation underscores the importance of viewing consciousness as a continuum rather than a rigid binary between waking and sleeping states. Sleep disruptions can destabilize cognitive and emotional boundaries, giving rise to dissociative phenomena, while dissociation itself may perpetuate sleep problems. Recognizing this interconnection allows clinicians to expand treatment strategies beyond trauma processing alone, incorporating sleep regulation as a key component of recovery. Ultimately, improving sleep may help restore coherence in consciousness, reducing the distressing experiences of fragmentation that define dissociation.


