For decades, psychiatric disorders such as depression, schizophrenia, and bipolar disorder were predominantly viewed through the lens of neurotransmitter imbalances. However, mounting evidence reveals that neuroinflammation—the brain’s immune response to various insults—plays a critical role in the onset, progression, and severity of many psychiatric conditions. Far from being a passive background process, neuroinflammation actively shapes cognition, emotion, and behavior, offering a new perspective on mental health and illness.
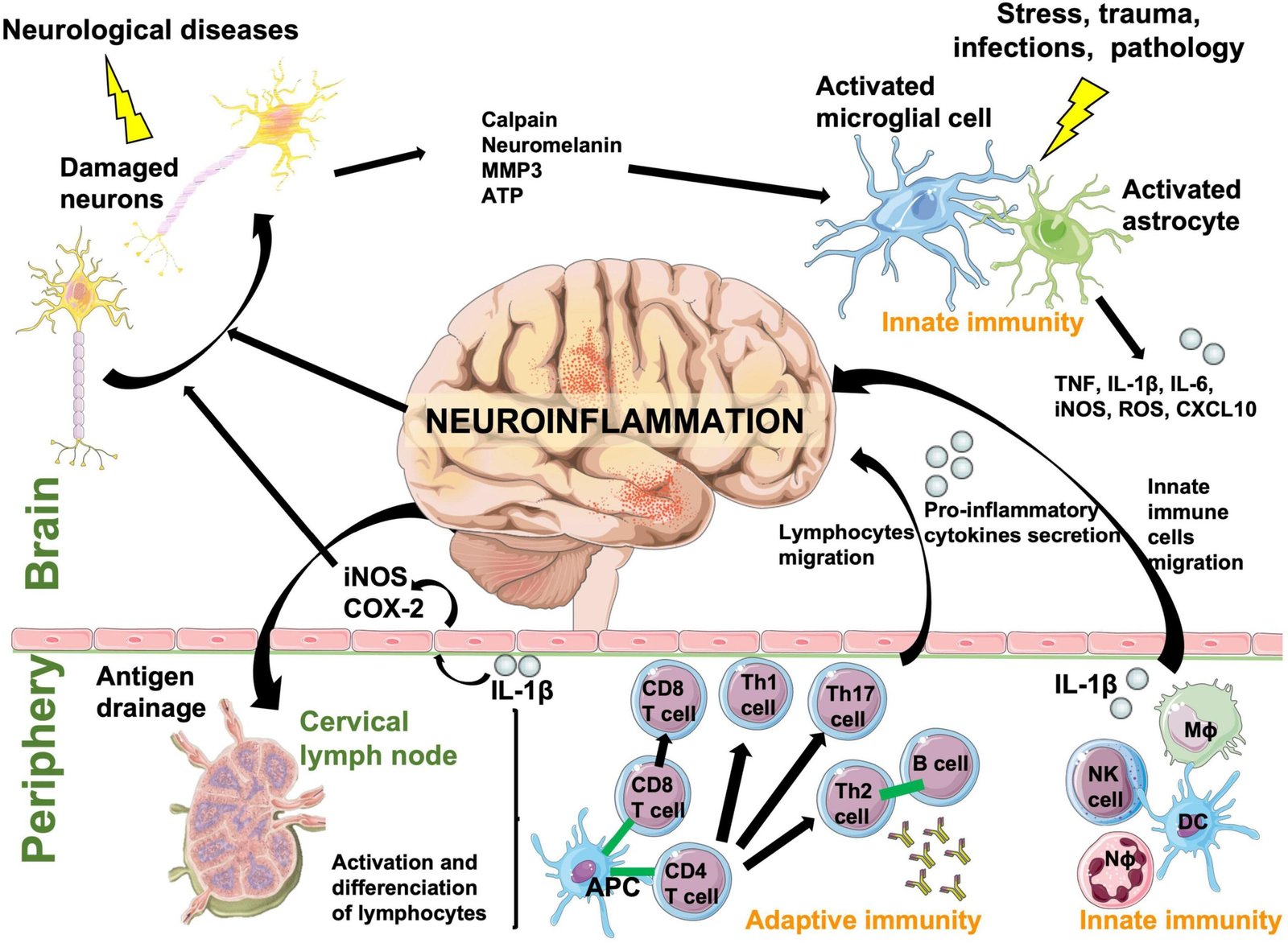
Neuroinflammation involves the activation of microglia and astrocytes, the brain’s resident immune cells. While normally protective, these cells can become chronically activated in response to infection, trauma, stress, or genetic vulnerability. Persistent activation leads to the release of pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1 beta (IL-1β). These molecules can cross the blood-brain barrier or alter neural signaling, resulting in changes to neurotransmitter systems and neural plasticity.
In major depressive disorder, elevated inflammatory markers are consistently observed. Patients with treatment-resistant depression, in particular, show higher levels of C-reactive protein (CRP) and cytokines compared to treatment-responsive individuals. These findings suggest that inflammation may underlie certain subtypes of depression, particularly those characterized by fatigue, anhedonia, and cognitive slowing. Anti-inflammatory agents, such as NSAIDs or cytokine-targeting drugs, are being investigated as adjunctive treatments for resistant depression.
In schizophrenia, neuroinflammation has been linked to abnormal neurodevelopment and synaptic pruning. Microglial overactivation may result in excessive elimination of synapses, contributing to cognitive impairment and negative symptoms. Elevated cytokine levels in first-episode psychosis further support the hypothesis that immune dysregulation plays a role in the early stages of the disorder.
In bipolar disorder, episodes of mania and depression have been associated with fluctuating inflammatory markers, suggesting that neuroinflammation may contribute to mood instability. Similarly, in autism spectrum disorder, evidence indicates that prenatal or early-life inflammation may alter brain development, increasing susceptibility to neurodevelopmental abnormalities.
The connection between stress and neuroinflammation further highlights its relevance in psychiatry. Chronic psychological stress activates the hypothalamic-pituitary-adrenal (HPA) axis, elevating cortisol levels and promoting inflammatory responses. Over time, this process can sensitize neural circuits, perpetuating both psychiatric symptoms and vulnerability to relapse.
Therapeutically, targeting neuroinflammation represents an emerging frontier. Anti-inflammatory pharmacological agents, lifestyle interventions (such as diet, exercise, and sleep optimization), and even microbiome-targeted therapies show promise in reducing psychiatric symptoms by addressing their inflammatory underpinnings. Importantly, not all patients with psychiatric disorders exhibit elevated inflammation, highlighting the need for personalized approaches based on biomarker assessment.
In conclusion, neuroinflammation provides a unifying framework that links immune dysregulation with psychiatric illness. It challenges traditional neurotransmitter-focused models, emphasizing that mental health is deeply intertwined with systemic and neural immune processes. Future psychiatry is likely to embrace an integrative paradigm—one that considers inflammation, immunity, and environmental influences alongside neurochemistry—paving the way for more effective and individualized treatments.


