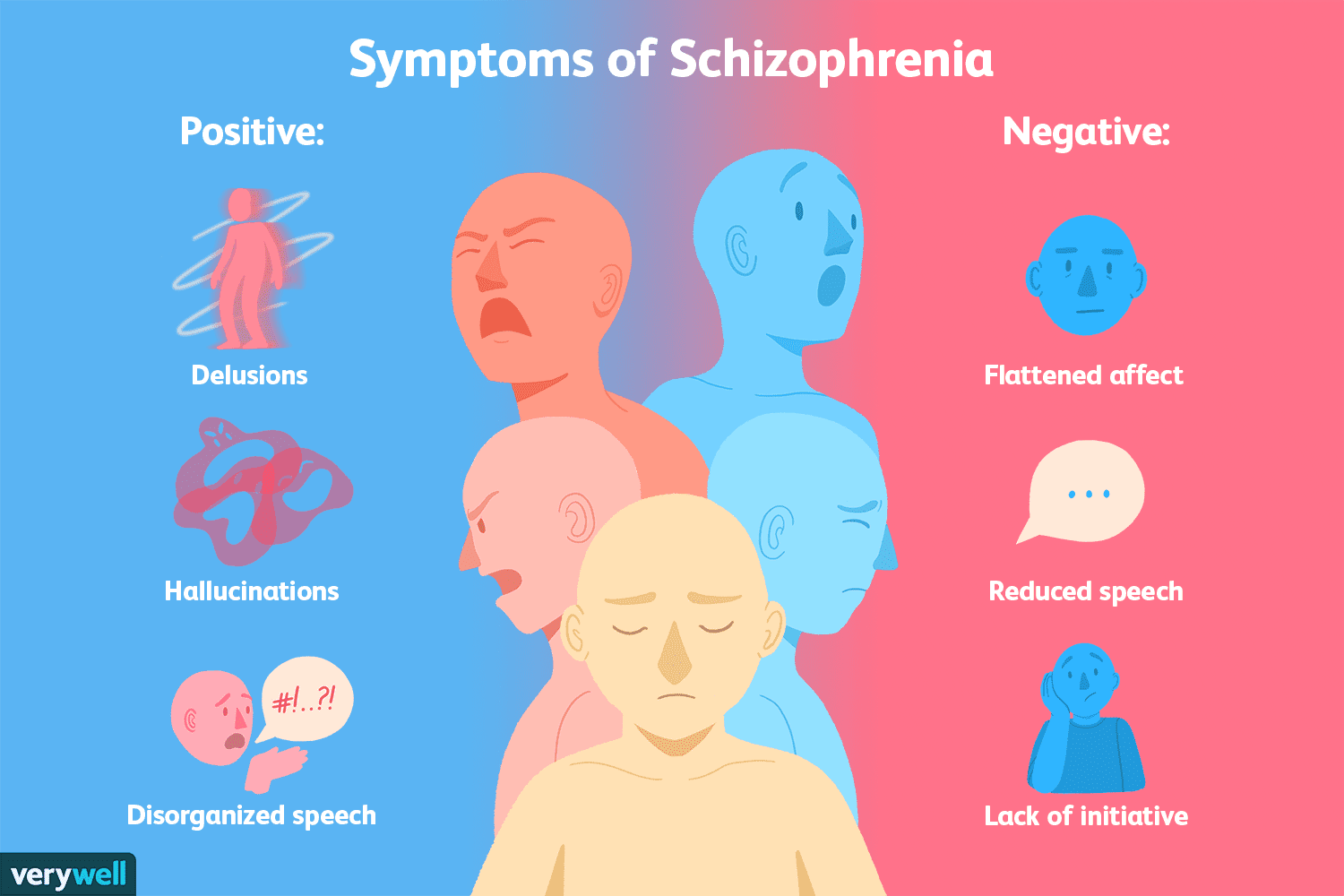
Schizophrenia is often recognized by its most conspicuous features: hallucinations, delusions, and disorganized speech or behavior. These positive symptoms dominate clinical and public perception of the disorder. However, there exists a set of negative symptoms—subtle, persistent, and often overlooked—that can be far more disabling in daily life. Negative symptoms include emotional blunting, reduced motivation (avolition), diminished speech output (alogia), social withdrawal, and anhedonia (the inability to experience pleasure). Despite their clinical significance, these symptoms are frequently underrepresented in research and popular discourse, earning them the label of the “silent symptoms” of schizophrenia.
Negative symptoms are particularly challenging because they are less responsive to traditional antipsychotic medications, which primarily target positive symptoms through dopaminergic modulation. As a result, patients may experience persistent functional impairment despite adequate control of hallucinations or delusions. Emotional blunting, for instance, reduces the capacity for normal affective expression, making interpersonal interactions difficult. Social withdrawal and avolition can prevent patients from engaging in work, education, or social activities, significantly decreasing quality of life.
Recent research suggests that negative symptoms may stem from complex neurobiological mechanisms, including dysregulation in the prefrontal cortex, hypoactivity in mesocortical dopamine pathways, and alterations in glutamatergic neurotransmission. These deficits impact cognitive and executive functions, compounding the challenges imposed by social and emotional withdrawal. Furthermore, environmental factors, such as early life stress or social isolation, may exacerbate negative symptoms by influencing brain development and neural connectivity.
One of the key challenges in diagnosing and treating negative symptoms is their subtlety. Unlike hallucinations or delusions, which are observable and easily reported, negative symptoms may be mistaken for depression, medication side effects, or lack of engagement. Clinicians must therefore carefully distinguish between these conditions through structured assessments and longitudinal observation. Tools such as the Scale for the Assessment of Negative Symptoms (SANS) or the Positive and Negative Syndrome Scale (PANSS) can aid in this evaluation, providing standardized measures of symptom severity.
Innovative therapeutic approaches are emerging to address these silent symptoms. Psychosocial interventions, including cognitive behavioral therapy, social skills training, and vocational rehabilitation, have shown promise in enhancing functional outcomes. Additionally, newer pharmacological strategies targeting glutamatergic and cholinergic systems are being investigated, aiming to directly improve negative symptomatology. Research into the role of inflammation and immune dysregulation also suggests potential novel avenues for intervention.
In conclusion, negative symptoms in schizophrenia represent a critical yet frequently overlooked dimension of the disorder. They profoundly affect patients’ daily functioning and quality of life, often persisting even when positive symptoms are controlled. Greater awareness, early detection, and comprehensive treatment strategies that integrate pharmacological and psychosocial approaches are essential to addressing the silent struggles of individuals living with schizophrenia. Recognizing and targeting these symptoms is not only crucial for clinical management but also for improving long-term social, occupational, and emotional outcomes.


